1. Who is dying in Italy?
Italy is now by far and away the country worse affected by the coronavirus, with 69,176 confirmed cases of infection and 6,820 deaths, the latter figure more than double the whole of China, with only 8,326 people recovered, and 3,393 currently in a serious or critical condition. As of today, Tuesday, 23 March, that’s almost 1 in 10 infected people dying in Italy. Last week the UK press universally reported that up to 7.9 million people could be hospitalised with the virus in the UK, so at this percentage of fatalities that’s nearly 780,000 people dead!
Okay, slow down, take a breath, start thinking again. Now, let’s have a look at the facts. I know this crisis has already gone far past that, and nobody cares about facts these days anyway, least of all those demanding the government — the government! — tell them the truth. But stay with me.
Italy has the second oldest population in the world after Japan. The median age is 47 — seven years older than in the UK — and a massive 23 per cent of the population is over 65, some 13.9 million people, compared to 18 per cent in the UK. So what? You ask. There’s a Coronavirus Disinformation Test doing the rounds on Facebook, and one of its supposedly correct answers is that the virus affects all ages, and not just the old. Well, yes, it does, but let’s look at the facts about the deaths in Italy.
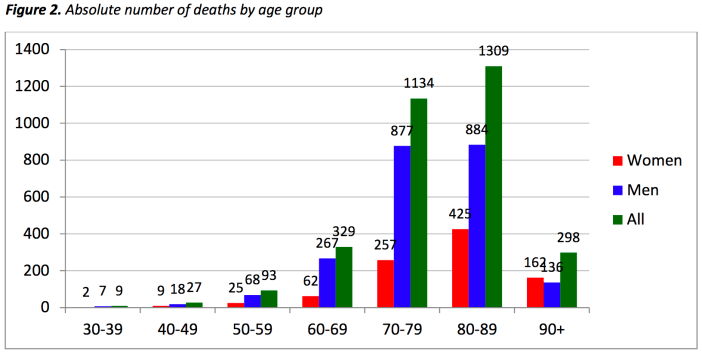
According to the most recent figures from the Istituto Superiore di Sanitá, the median age of those hospitalised by coronavirus disease 2019 (COVID-19) in Italy is 65, with 75 per cent of those infected over the age of 50. Even more indicative, 85.6 percent of those who have died were over 70, with a median age of 80. Unsurprisingly, the majority suffered from underlying health problems. More than 99 per cent of Italy’s deaths from COVID-19 had previous medical conditions. Nearly half suffered from at least three prior illnesses, and over a quarter had either one or two previous conditions. Nearly 74 per cent had high blood pressure, 34 per cent had diabetes and 30 per cent suffered from heart disease. In contrast, as of 20 March, when Italy had 41,000 confirmed cases of the illness and 3,200 deaths, only 36 people under 50 had died of COVID-19. 7 of the 9 victims under 40 had serious existing medical conditions.
So, what does this mean? Severe Acute Respiratory Syndrome Coronavirus 2 (SARs-CoV-2) is undoubtedly a flu pandemic, with the extent of infection in the UK not known until the government starts testing the wider population, rather than leaving it to the 13 per cent of UK customers with private health care. Until that happens, we don’t know how many of us have the virus, with the current estimate of 8,000 cases a fraction of our European neighbours. But the figures coming out of Italy show that overwhelmingly COVID-19, the disease coronavirus causes, kills the old and the sick. As recently as 1947, the average age at which men in the UK died was 65. Since then we’ve increased our life expectancy to nearly 80 for British males; but although we live longer with the help of vaccines and drugs that protect us from what used to kill us, until we find a vaccine for SARs-CoV-2 it will continue to kill the elderly, just as rubella, the measles, chicken pox, diptheria, tuberculosis, tetanus, polio, and all the other things we’re now vaccinated against once did.
2. Who is vulnerable in the UK?
Unless we live in total isolation from each other until a vaccine is found — which economically is impossible — eventually a lot of us will contract the virus, fall sick, recover, and develop a level of immunity to it. But let’s stop there again and look at what ‘a lot’ means. At 1,144 recorded cases in every million of the population, Italy has by far and away the highest level of infection per capita: 20 times higher than in China, three times what it is in Germany. But in a population of over 60 million, that is still 1 in every 875 people.
To draw a comparison, in the London Borough of Lambeth, where I live, that’s the equivalent of 397 people out of a borough population of nearly 347,500 that would contract the virus if we reach the level of infection in Italy. So, if our population were as old as Italy’s — which it isn’t — and the percentage of deaths to recorded cases as high, 40 of these people would die. 35 of them would be over 70, with an average age of 80, with several existing health problems. Remember, this figure is based on the worst existing conditions in the world at the moment.
If the UK population does what it’s told and stays at home for the next two months until everybody that has the virus now has either recovered or died, unless we continue to quarantine the entire country until a vaccine is found, with nobody entering and nobody leaving and all imported goods disinfected — all of which is also impossible — sooner or later the infection will start again, and we’ll be back where we are now. That’s not quite right, as hopefully we’ll be closer to finding a vaccine; but nobody can say when that will be, with the latest estimate being summer 2021. One way or another, a lot of us are going to catch SARs-CoV-2. But if we drop these comparisons to the worst-case scenario, the World Health Organisation estimates that in 80 per cent of cases of infection we will suffer mild symptoms, in 15 per cent severe symptoms, and the coronavirus disease will be critical to 5 percent of those infected. Only in this latter category can the coronavirus lead to death.
As I argued previously in COVID-19 and Capitalism, the measures being passed by the UK government in response to the coronavirus have little to do with its threat to our health, which to the 82 per cent of the UK population that is under 65 and in good health is almost non-existent beyond a dose of the flu. People over 60 should take care, and not go to work or take public transport, and the rest of us should do our best not to have unnecessary contact with them in case we have the virus — much as most of us already do, I’d imagine, if we’ve caught seasonal flu. There is some logic to spreading out the infection of the UK population over as long a period as possible, since the NHS already enters into a crisis every winter for lack of staff and funding due to cuts by successive Neo-liberal governments, though presumably there’s only so long a government can suspend the economy of the country before the whole thing breaks down.
But the current ‘shutdown’ of the UK, sending workers home for the foreseeable future with a fuzzy promise that their employers will be compensated for 80 per cent of their salaries, closing down venues and events in which people can meet, and passing legislation that gives emergency powers to the police to enforce martial law for the next two years and more, is about reducing and recouping the huge financial losses the global suspension of trade and the resulting crash of the stock markets are costing the wealthiest people in the world — almost all of whom, unsurprisingly, are over 60 and have private health insurance — at the expense of the rest of us.
3. How many are dying from the coronavirus?
Last week the Chief Scientific Adviser, Sir Patrick Vallance, told the government that the number of anticipated deaths from COVID-19 in the UK would depend on the government’s actions. According to estimates by Imperial College London, 510,000 people will die if we do nothing; if we slow the spread of the coronavirus, isolating the vulnerable and those with symptoms, it was 250,000; but if we shut the UK down, it could be as little as 20,000. In comparison, Vallance told the Health Select Committee, an average of 8,000 people would be expected to die of seasonal flu in any given year. It’s on this official estimated increase in the number of deaths from COVID-19 that the government has issued its extralegal shutdown of the UK and Parliament has passed the human rights-suspending Coronavirus Act.
However, the figures quoted by the Chief Scientific Adviser are not strictly accurate. First, the average of 8,000 deaths is from an estimate made by Public Health England in 2014, and which has now been withdrawn from the UK government’s website because it is over 4 years old. The more recent estimate by Public Health England based on the last five years is that the average number of deaths from seasonal flu in England alone is 17,000 every year. Even these figures vary hugely. In 2018-19 it was 1,692, while in 2014-15 it was 28,330 — a figure that dwarfs anything we’ve seen from COVID-19 so far. So there’s no way to know with any accuracy until it happens. This alone raises questions about the impartiality of this advice from Sir Patrick Vallance.
But second, and even more suspiciously, while the figure of 8,000 deaths from seasonal flu quoted by the Chief Scientific Adviser was for excess deaths, over and above the average number of deaths in the UK in a year, his estimate of the number of deaths from COVID-19 includes the large number of the deaths we would otherwise expect to see. So whatever the number of people who would have died in the UK this year if SARs-CoV-2 hadn’t arrived on these shores, the failure to distinguish between predictions of the number of deaths from COVID-19 in the UK — whether that’s 20,000, 250,000 or 500,000 — and the number of people over 65 that would have died anyway of high blood pressure, heart disease, diabetes, dementia, Alzheimer’s, pneumonia, bronchitis, liver disease, cancer or a stroke is something that’s been deliberately ignored by the government in the increasingly alarmist estimates being circulated by the media as justification for the rapid removal of our civil liberties and human rights. It’s too late now, but Professor Neil Ferguson, the Imperial College scientist whose research justified the government’s shutdown of the UK, has now retracted his initial estimates, saying that fatalities from COVID-19 could be ‘substantially lower’ than 20,000, and that between one-half and two-thirds will have died anyway because of their age or from underlying conditions.
According to the Office for National Statistics, 616,014 people died in the UK in 2018, and the vast majority fit the age and health profile of the vast majority of the victims of COVID-19. In Italy, that means dying at an average age of 80, with 99 per cent of fatalities having existing health conditions. That’s a year higher than the average age at which men die in the UK today, and three years lower than for women. But while many of the official victims of the pandemic have died with the virus in their body, no estimates have been made by the British authorities of how many will die of the coronavirus, and how many will die of the numerous other illnesses and diseases that carry off the elderly and the sick every year. Of the 527,164 people who died last year in England and Wales, 33,834 people died from respiratory diseases; 87,492 people were between the age of 65 and 74; 149,669 between the age of 75 and 84, and 208,681 over the age of 85. That’s nearly 446,000 people over 65 who died in England and Wales a year before the coronavirus arrived in the UK. How many with this age and health profile will officially die this year from COVID-19?
To take a comparative sample, in the four weeks between 2 and 29 March last year, 41,743 people in England in Wales died out of a total population of 59 million, and 35,149 of them were over 65. In Italy, with a population of 60 million, over the same period this year 9,879 people have officially died while testing positive for SARs-CoV-2, and around 8,500 of them were over 70. However — and this can’t be too emphasised — only 12 per cent of death certificates have shown a direct causal relation to COVID-19. The real measure of the death rate is those dying from pulmonary diseases, and the air quality in Northern Italy, which is the worst in Europe, is a contributing factor to the increased mortality rate, just as it was in Wuhan.
According to a study published in 2019 in the International Journal of Infectious Diseases, in Italy over the winter season of 2016-17, some 24,981 excess deaths were attributable to influenza-related illnesses; the previous year, 2015-16, there were 15,801; the year before that, 2014-15, there were 20,259. Most of these deaths were among people over 65, who made up 77.7 per cent in 2016-17, 96.1 per cent in 2014-15. ‘The observed excess of deaths is not completely unexpected,’ the study therefore concluded, ‘given the high number of fragile very old subjects living in Italy.’
We’re so distanced from death in the capitalist world — whether our own deaths or those we inflict in far greater numbers on other countries — that sudden public awareness of our mortality rate throws us into the panic we’re witnessing now. As I said in my earlier article on the coronavirus pandemic, the perception of death the state apparatus allows us to have is determined by how it serves capitalism.
4. The class war in mortality
Although not as high as Italy’s 23 per cent, the 18 per cent of the population in the UK that is now over 65 has changed the political landscape over the past decade. A new political divide has opened in the UK between those who own their own home and those who don’t have a chance of ever doing so; between those who vote for government subsidies that maintain the value of their property and those who want policies that will bring housing costs down; between those who want the best health service their money can buy and those who want a public health service accessible to all. Since all our Parliamentary parties are committed to the increased marketisation of housing provision, the continuing financialisation of the property market, and the ongoing privatisation of all our public services — and not just the NHS — we should be wary of mapping this age divide onto our voting preferences; but 64 per cent of voters over 65 in the 2019 general election voted for the Conservative Party.
As the number of homeless people in the UK over the past decade has grown to 320,000, as food-banks have become the only way to eat for millions of working-class families, as single mothers on the breadline have had their benefits cut by £60/week, as thousands of the disabled have been deprived of Employment and Support Allowance and either taken their own lives or simply starved to death, and as funding for the NHS has been cut to the bone to facilitate its privatisation, anyone who voted for Cameron, May and Johnson to be Prime Minister of the UK will get little sympathy from me. Unfortunately, it’s the 35 per cent of over 65s who didn’t vote Conservative, and the as many more who didn’t vote at all, that are likely to suffer the most from coronavirus disease 2019. This is the time to recall that the government didn’t commit £350 billion of public money to rescue packages as an estimated 120,000 people — most of them over 60 — died as a result of austerity cuts to benefits and health services implemented by successive Conservative Chancellors since 2010.
As a direct result of these fiscal policies, life expectancy in the UK over the past decade has stopped rising for the first time since the 1890s, and life expectancy for the poor has actually dropped. For years now, the age gap in mortality between the rich and the poor has been widening. According to the British Medical Journal, it is now nearly 10 years for men in England — with the rich dying at an average age of 84 years, and the poor at 74. Without their private health care, their private pensions annuities, their organic health-food diets, their private gym memberships, their second home in the Cotswolds, their four holidays a year in the sun, their Indian nurses, Brazilian cleaners, Filipino maids and French au pairs, above all without their stress-free, financially comfortable retirement, the rich die at the same age as the rest of us. If, like me, you’re a historical materialist, you understand that every social phenomenon, including a flu pandemic, is first and foremost an economic phenomenon, and SARs-CoV-2 is proving this to be the case — in its causes, its transmission, its effects, and our responses to it.
What these facts and figures about SARs-CoV-2 and COVID-19 show is that this pandemic is nature overcoming all the drugs we pump into our bodies from birth to stave off the inevitable. Sooner or later we’ll invent a new vaccine and the life expectancy of the rich will go up again; but until we do, our current panicked response is more about the resignation of the working classes, the fear of the middle classes and the outrage of the rich that, with all our technology and wealth and apparent ability to bend nature to our will, we still can’t beat death. Just as the global environment is busy correcting that particular assumption of capitalism, so too is the coronavirus.
In my next article on the pandemic I’ll be looking at how the UK government is using this resignation, fear and outrage for its own ends, and how, by giving free reign to our panic, we are willingly inserting our wrists into the manacles that will bind us for years to come.
Simon Elmer
Architects for Social Housing
Further reading:
Lockdown: Collateral Damage in the War on COVID-19
Manufacturing Consensus: The Registering of COVID-19 Deaths in the UK
Giorgio Agamben and the Bio-Politics of COVID-19
Good Morning, Coronazombies! Diary of a Bio-political Crisis Event
Coronazombies! Infection and Denial in the United Kingdom
Language is a Virus: SARs-CoV-2 and the Science of Political Control
Architects for Social Housing is a Community Interest Company (no. 10383452). Although we occasionally receive minimal fees for our design work, the majority of what we do is unpaid and we have no source of public funding. If you would like to support our work financially, please make a donation through PayPal:
![]()

2 thoughts on “Sociology of a Disease: Age, Class and Mortality in the Coronavirus Pandemic”