Table of Contents
Part 1. Adverse Drug Reactions and Deaths
-
- What is a COVID-19 ‘Vaccine’?
- Adverse Drug Reactions to COVID-19 ‘Vaccines’
- Deaths Following Injection with a COVID-19 ‘Vaccine’
- Overall Mortality in the UK Biosecurity State
It’s been nine months now since, in my article Lies, Damned Lies and Statistics: Manufacturing the Crisis, I analysed the statistics on official ‘COVID-19 deaths’ published by the institutions responsible for justifying the regulations and programmes of the UK biosecurity state. These include the Office for National Statistics, the National Health Service and Public Health England. Together with concerned reports from medical bodies, including Cancer Research UK, the British Heart Foundation and the Alzheimer’s Society, these statistics strongly suggested that at least half the 80,000 deaths attributed to COVID-19 in 2020 resulted from the withdrawal of medical diagnosis, treatment and care under lockdown restrictions. However, this is a conservative estimate, and doesn’t include the 20,000 excess deaths in care homes last year swept under the COVID-19 carpet. I’m pleased to relate that my article has been visited over 57,000 times on our website, which shows, if nothing else, that there is a continued desire among the public to know what is actually going on, and an ongoing refusal to accept the increasingly transparent lies we continue to be told by those awarding themselves increasing power and authority over our lives.
Since then, the programmes of the UK biosecurity state have expanded into mandating injection with COVID-19 ‘vaccines’ as a condition of employment for care workers from 11 November and, more recently, they were proposed as a condition of attending lectures for students in higher education. This proposal has now been dropped, but judging by the expansion of such discriminatory dictates in other countries such as Ireland, France and Greece, there is little doubt the UK Government and its state apparatus will follow suit in mandating medical intervention for more and more of the population, with the Secretary of State for Health and Social Care this week threatening to mandate them for all NHS staff and social care workers. And while the requirement to carry proof of such medical treatment in the form of digital biosecurity monitoring called ‘vaccine’ passports is yet to receive the force of primary legislation, statutory regulation and police enforcement, it is already being ‘rolled out’ — as the imposition of these measures is described nowadays — through bullying and incentivising both private businesses and public institutions into making them a condition of employment. The newly-branded ‘NHS COVID Pass’ is already required to travel abroad and enter some venues in the UK. Last week, the Scottish Parliament voted for ‘vaccine’ passports to be made a condition of entry to entering theatres, exhibitions, nightclubs, concerts, festivals, stadiums and other large venues from 1 October; and this week the Welsh Assembly is expected to follow its undeclared policy of always outdoing Westminster in virtuous authoritarianism. And although the Secretary of State has declared that ‘vaccine’ passports won’t be imposed in England in September, as they were threatened to be until recently, the Government has not ruled out their imposition in the future as part of its ‘COVID-19 Response: Autumn and Winter Plan’.
Now, therefore, seems a good time to return to the statistical records of what has been happening over the past 9 months, to look not just at the number of deaths attributed to COVID-19 in order to justify the UK ‘vaccination’ programme but also, and primarily, at the adverse drug reactions, including death, recorded following — if not necessarily resulting from — this unprecedented programme of increasingly enforced medical intervention in the bodies of the UK population. If we are to believe the official figures, the UK has one of the highest levels of compliance with this programme of any country in the world, with a purported 92.1 million doses of a COVID-19 ‘vaccine’ administered, of which 72.4 per cent of the population have received at least one dose and 65.4 per cent are ‘fully vaccinated’. At the same time, the demonstrations of non-compliance, which began to grow in size in the spring of 2021, and for several months in succession put over a million people on the streets of London, indicates that the war is not yet lost, and may even be turning. Certainly, the drive to bully, shame, ridicule, threaten and now compel the British people to take, and keep on taking, the growing number of ‘vaccine’ brands granted temporary authorisation by the Medicines and Health products Regulatory Agency (MHRA) has not let up, but rather intensified.
When I first started writing about the coronavirus crisis in April 2020, and even as I tried to document the rapid implementation and expansion of the UK biosecurity state over the year that followed, I was publishing information and analysis that was hidden, hard to access and often not being published elsewhere. Over the past nine months, the greater availability of information on how and to what ends the biosecurity state is being implemented has raised awareness of the extent of the lie being perpetrated; but it has done little to halt the collaboration of the UK Government, its state institutions, British businesses and the British people in the New World Order that has been constructed with such extraordinary rapidity. Today, eighteen months into the Fourth Industrial Revolution that has swept through the former liberal democracies of the West, we stand at the threshold of a digitally monitored and controlled totalitarianism towards which we have been sleepwalking since the manufactured crisis of March 2020, and those who understand best what is happening and to what ends believe our next step will be irreversible. Before we take it, therefore, I have assembled just some of the latest evidence in our defence against the UK ‘vaccination’ programme, the presentation of which will, I hope, convince enough of us to stop, turn around and start the long and difficult march back to recovering our rights, our freedoms, our bodies and, indeed, our minds from the chains of the UK biosecurity state.
1. What is a COVID-19 ‘Vaccine’?
Rachel McKinney, a healthy 35-year-old mother of two children and part-time manager in a nursing home, was injected with her first dose of the Pfizer ‘vaccine’ in late December 2020, followed by a second dose in January 2021. A month later, she started showing signs of having had a stroke, with symptoms that included confusion and slurred speech. Having been advised to attend Stepping Hill Hospital in Stockport, an MRI scan showed she had inflammation of the brain. However, due to coronavirus-justified restrictions, her family were not permitted to visit her. A week later, Mrs. McKinney was transferred to Salford Royal Hospital, where she was diagnosed with Acute disseminated encephalomyelitis (ADEM), a rare inflammatory condition that affects the brain and spinal cord. Despite this, the hospital continued to refuse to allow her family to visit her. Alone and frightened, Mrs. McKinney quickly lost her speech, movement down one side of her body, and was extremely disoriented and confused about what was happening to her.
After weeks alone in hospital, Mrs. McKinney took a turn for the worse. The plasma exchange treatment, which doctors hoped would give her immune system a chance to fight back, had not been successful, and she had multiple seizures. She was put into a medically induced coma, and spent two weeks on a ventilator in intensive care. On 24 March, her family were told Mrs. McKinney had developed a very rare and aggressive form of multiple sclerosis and that nothing more could be done to help her. On 3 April, 46 days after she had entered hospital and a few days after doctors made the decision to turn off her life-support machine, Mrs. McKinney died, unaware that her husband and mother were by her side.
In June 2020, 3 months into the coronavirus crisis in Europe, the definition of ‘herd immunity’ being espoused by the World Health Organisation (WHO) was as follows:
‘Herd immunity is the indirect protection from an infectious disease that happens when a population is immune either through vaccination or immunity developed through previous infection.
‘This means that even people who haven’t been infected, or in whom an infection hasn’t triggered an immune response, are protected because people around them who are immune can act as buffers between them and an infected person. The threshold for establishing herd immunity for COVID-19 is not yet clear.’
By October 2020, however, the WHO was employing an entirely new definition, according to which herd immunity through infection of a proportion of the population was now explicitly rejected not only as scientifically ’problematic’ but also as ‘unethical’:
‘“Herd immunity”, also known as “population immunity”, is a concept used for vaccination, in which a population can be protected from a certain virus if a threshold of vaccination is reached. Herd immunity is achieved by protecting people from a virus, not by exposing them to it.
‘Vaccines train our immune systems to create proteins that fight disease, known as ‘antibodies’, just as would happen when we are exposed to a disease but — crucially — vaccines work without making us sick. Vaccinated people are protected from getting the disease in question and passing it on, breaking any chains of transmission.
‘Attempts to reach “herd immunity” through exposing people to a virus are scientifically problematic and unethical. Letting COVID-19 spread through populations, of any age or health status will lead to unnecessary infections, suffering and death.’
Following suit with this demonstration of George Orwell’s maxim that ‘who controls the past controls the future, who controls the present control the past’, Merriam-Webster, the US online dictionary, employed the following definition of the word ‘vaccine’ before the coronavirus crisis:
‘A preparation of killed microorganisms, living attenuated organisms, or living fully virulent organisms that is administered to produce or artificially increase immunity to a particular disease.’
Then, in January 2021, as the COVID-19 ‘vaccination’ programme was initiated around the world, this definition was expanded to include the following:
‘A preparation that is administered (as by injection) to stimulate the body’s immune response against a specific infectious agent or disease: such as:
a: an antigenic preparation of a typically inactivated or attenuated pathogenic agent (such as a bacterium or virus) or one of its components or products (such as a protein or toxin);
b: a preparation of genetic material (such as a strand of synthesized messenger RNA) that is used by the cells of the body to produce an antigenic substance (such as a fragment of virus spike protein).’
Helpfully, as examples of how to use this new definition of ‘vaccine’ in a sentence, the dictionary suggested the following references to the pharmaceutical companies and bio-technologies responsible for its acceptance:
‘Moderna’s coronavirus vaccine . . . works by injecting a small piece of mRNA from the coronavirus that codes for the virus’ spike protein. . . . mRNA vaccine spurs the body to produce the spike protein internally. That, in turn, triggers an immune response.
‘Viral vector vaccines, another recent type of vaccine, are similar to DNA and RNA vaccines, but the virus’s genetic information is housed in an attenuated virus (unrelated to the disease-causing virus) that helps to promote host cell fusion and entry.’
In a short space of time, therefore, the definition of what both herd immunity and a vaccine are, as well as the relation between them, had been changed to fit government policy on responding to SARS-CoV-2 by employing equally new products developed by the pharmaceutical industry.
More recently, another definition of the COVID-19 ‘vaccines’ temporarily authorised for use in the UK has emerged. On 6 August, 2021, Public Health England, the executive agency of the Department for Health and Social Care, published its 20th technical briefing under the title ‘SARS-CoV-2 variants of concern and variants under investigation in England’. And on its summary page it states:
‘PCR cycle threshold (Ct) values from routinely undertaken tests in England show that Ct values (and by inference viral load) are similar between individuals who are unvaccinated and vaccinated.’
As a non-scientist, it’s not clear to me how, 18 months into this ‘pandemic’, the UK medical profession has been unable to come up with a more accurate test of infection or cause of death than the reverse transcription-polymerase chain reaction (RT-PCR) test that has been denounced around the world as ‘unfit for purpose’ and will be discontinued in the US as a diagnostic tool for SARS-CoV-2 as of next year, yet we are apparently able to diagnose variants from genome sequencing the same swab samples of hundreds of thousands of hospital patients. But be that as it may, the PHE report is focused on variants of SARS-CoV-2 in England in the 6 months between 1 February and 2 August 2021, of which there have been 150,541 so-called ‘cases’ of the Alpha variant and 300,010 ‘cases’ of the Delta variant that have attended emergency care in hospitals in England. These make up all but 2,527 of the apparently ever-increasing variants identified as present in the UK.
First, in Table 5 on page 18 (below), the briefing reports that, of the 300,010 patients attending emergency care that were diagnosed with the Delta variant of SARS-CoV-2, 151,054 (just over half) were ‘unvaccinated’; and of the 148,956 (just under half) who had received a COVID-19 ‘vaccine’, 47,008 had received 2 doses, 46,089 had received 1 dose at least 21 days previously, and 24,018 within 21 days. What these figures suggest is that, far from reducing the symptoms of COVID-19, particularly those severe enough to warrant a visit to emergency care, the COVID-19 ‘vaccines’ make little or no difference.

The most interesting part of this briefing, however, is in section 1.7, titled ‘Vaccination’. Given only a single page in a 43-page report and removed from subsequent technical briefings, PHE makes the following statement about the difference in the detected viral load of those who have and have not been ‘vaccinated’. This is measured by the different cycle threshold (Ct) values at which the RT-PCR test registers a ‘positive’, with the higher the Ct value, the lower the viral load. This is what PHE reports:
‘In the NHS Test and Trace (NHSTT) case data, the mean and median lowest Ct values for all cases with Delta, where Ct data are available, since the 14 June 2021 are similar, with a median of 17.8 for unvaccinated and 18.0 for those with 2 vaccine doses. This means that whilst vaccination may reduce an individual’s overall risk of becoming infected, once they are infected there is limited difference in viral load (and Ct values) between those who are vaccinated and unvaccinated. Given they have similar Ct values, this suggests limited difference in infectiousness.’
Below this statement, a chart (below) shows Ct values between September 2020 and July 2021 in people who have been diagnosed with the Alpha variant (shown in red, yellow and brown) and the Delta variant (shown in green, blue and purple). The three colours for each variant show Ct values for those who are ‘unvaccinated’ (respectively, brown and purple), those with 1 dose of ‘vaccine’ injected more than 21 days ago (yellow and blue), and those with 2 doses of ‘vaccine’ more than 21 days ago (red and green).
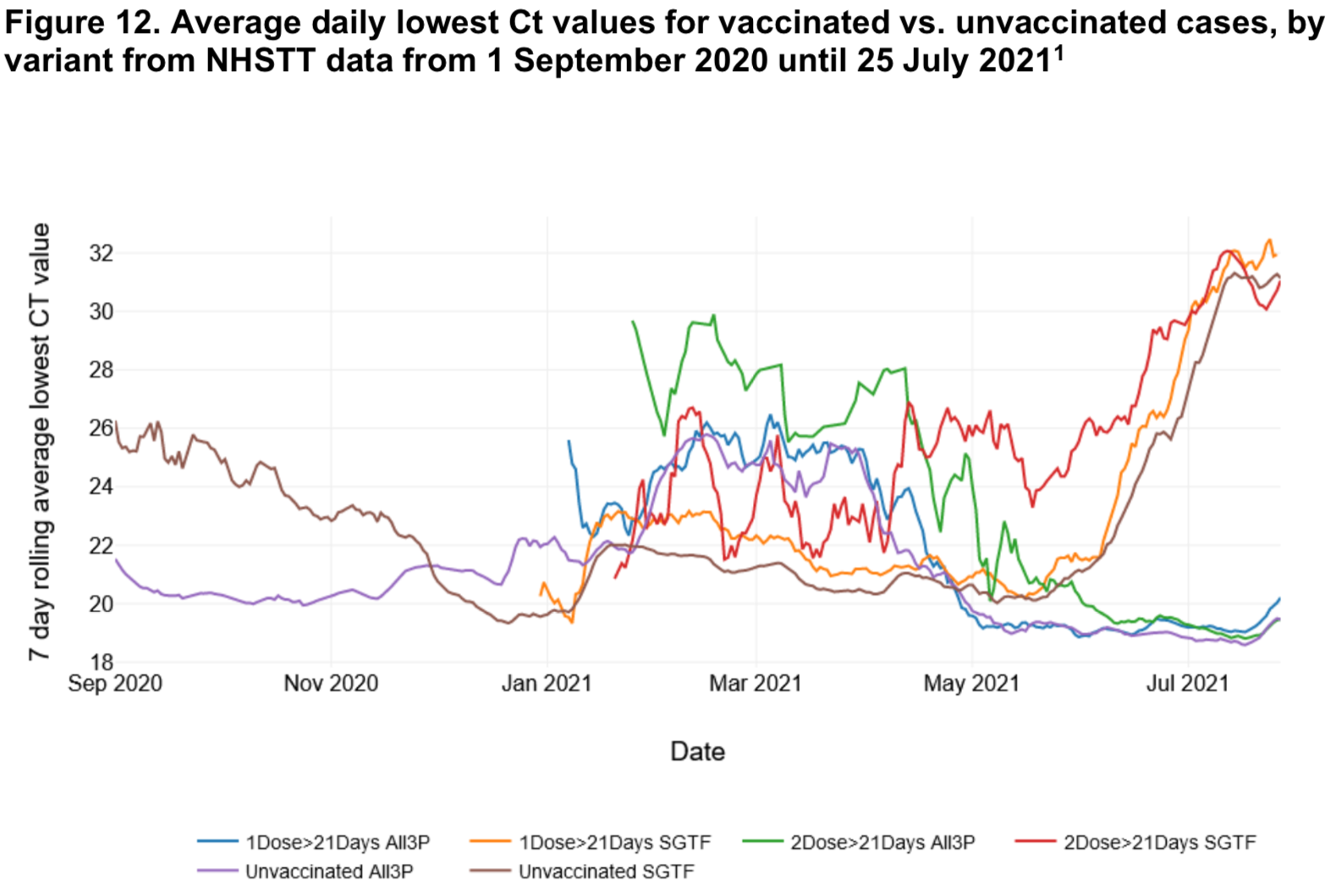
These comparative Ct values show that, in July 2021, to be officially diagnosed as a ‘case’ of the Alpha variant of SARS-CoV-2, the cycle threshold needs to be between 31 and 32, at which the RT-PCR test has to amplify viral DNA well over 2 billion times and any virus detected, according to the Centre for Evidence-based Medicine at Oxford University, is dead and non-infectious; while for the Delta variant a ‘case’ requires a Ct value of between 19 and 20, at which a strand of viral DNA is amplified half a million times, and may actually indicate infectiousness. Importantly, though — as PHE hurriedly states without comment — whether the positive test is of someone who has been injected with one dose of a COVID-19 ‘vaccine’, two doses or none at all makes no difference to the viral load with either variant. What PHE doesn’t say in its briefing, therefore, but which is the logical conclusion to be drawn from these figures, is that the COVID-19 ‘vaccines’ that have been injected into the arms of 48 million people in the UK make no difference to the health impact of SARS-CoV-2, the viral load or its infectiousness.
Last week, PHE published its latest, 22nd technical briefing, under the same title, and the results of the UK ‘vaccination’ programme are even worse. In Table 5 on page 21 (below), it reports that, of the 492,528 attendances to emergency care diagnosed with the Delta variant, 27,993 had one injection with a COVID-19 ‘vaccine’ within less than 21 days; 80,877 had one injection 21 days or more before, and 113,823 had 2 injections in 14 days or more, when they were officially ‘fully vaccinated’. That makes 222,693 people attending emergency care who had some degree of vaccination diagnosed with the Delta variant of SARS-CoV-2. In comparison, 219,716 had been unvaccinated (with a further 50,119 unlinked to a ‘vaccination’ status). Once again, then, these figures show that partial or full ‘vaccination’ has made no difference to ‘infection’ with SARS-CoV-2, or at least to receiving a positive RT-PCR test, and, in fact, that the percentage diagnosed with this method was increasing among the so-called ‘vaccinated’.

The percentages get even worse, however, when we look at deaths within 28 days of a positive test (below). Of the 1,798 deaths of patients diagnosed with the Delta variant between 1 February and 29 August 2021, 16 died in less than 21 days of their first injection, 126 died 21 or more days after their first injection, and a massive 1,091 died 14 days or more after their second injection. In contrast, 536 patients diagnosed with the Delta variant were ‘unvaccinated’ (with a further 29 deaths that could not be linked to ‘vaccination’ status). This means that those known to be fully ‘vaccinated’ with a COVID-19 ‘vaccine’ constituted 60.7 per cent of all deaths from the Delta variant of SARS-CoV-2 since 1 February, a figure which rises to 68 per cent when including the partially ‘vaccinated’; while the ‘unvaccinated’ made up less than 30 per cent.

And so that it’s clear, this imbalance is not merely because a significantly higher proportion of the elderly have received the ‘vaccine’ and would therefore be expected to constitute a higher percentage of those dying. It’s an odd watershed, given that COVID-19 is overwhelmingly an underlying cause of death attributed to people dying over the age of 70; but of the 1,091 people who died after two injections, 1,054 were 50 years of age or older (97 per cent), while of the 536 who died without being ‘vaccinated’, 437 were 50 or over (81.5 per cent).
To the extent these figures can tell us anything about who is actually dying from COVID-19 and not merely being diagnosed with a positive RT-PCR test pre- or post-mortem for possibly infectious traces of one of the coronaviruses they have a high chance of being infected with in the hospital, they show us that, far from COVID-19 ‘vaccines’ providing 95 per cent ‘efficacy’ and other fabrications of the pharmaceutical companies’ inadequate, incomplete and fraudulent trials, whatever is in these experimental ‘vaccines’ is making the elderly and already ill more vulnerable, not less.
This is only a single example of the already extensive and rapidly growing evidence that the drugs authorised for use in the UK to combat the effects and spread of COVID-19 do neither, and cannot, therefore, be considered to be vaccines, even by the changed definition of what a vaccine can and should do. If the definition of a vaccine — through which alone, now, we are being permitted by the UK Government and its advisors to reach herd immunity to COVID-19 — is that those vaccinated with it are, according to the WHO, ‘protected from getting the disease in question and passing it on, breaking any chains of transmission’, then none of the COVID-19 ‘vaccines’ being injected into the people of Britain can with any medical accuracy be called a vaccine. For this reason, when using this word in the context of the COVID-19 ‘vaccination’ programme, I always place it in inverted commas, as I do throughout this article. So what, if they do not protect us from infection with SARS-CoV-2, stop its transmission to others, or lessen the severity of the symptoms of COVID-19 — including the chances of death — do these ‘vaccines’ actually do?
2. Adverse Drug Reactions to COVID-19 ‘Vaccines’
On 13 March, 2021, Paul Bainbridge, a 46-year-old software developer from the UK, had his first dose of a COVID-19 ‘vaccine’. To celebrate the event he announced it on his Facebook page with a photograph of himself surrounded by a rainbow and a blue heart saying ‘thank you NHS’. Three days later he confirmed that he had been injected with the AstraZeneca viral-vector ‘vaccine’, along with the information that he had what he called ‘a dodgy immune system’. Over two months later, on 29 May, Mr. Bainbridge declared himself ‘fully vaccinated’, presumably meaning that he had received his second dose. A friend, Paul Oxley, whose profile photo bore the same rainbow and heart, asked: ‘Are you glowing yet?’ In response, Paul wrote: ‘No. But I now have 3 arms and metal keeps sticking to me’. This mockery was typical of Mr. Bainbridge’s views. On 19 September, 2020, he posted a photograph of the anti-lockdown demonstration in Trafalgar Square — a demonstration in which I participated — with the comment: ‘Anti maskers and anti vaxxers at Trafalgar Square. Or as they are collectively known. A Karen of Ratlickers’. I’m not sure if this is accurate, but Wikipedia says that ‘Karen is a pejorative term for a white woman seeming to be entitled or demanding beyond the scope of what is normal.’ I guess a ‘ratlicker’ is fairly self-explanatory.
On 1 June, a few days after his second injection, Mr. Bainbridge posted a summary of his rapidly deteriorating health. On 30 May he had felt ‘pins and needles’ in his hands and feet. The next day he was ‘falling over’ and was sent by his GP to a hospital, where he had two spinal taps and was ‘diagnosed same day’. On 2 June he had ‘full body paralysis with the exception of right side of face’, and was put into an ‘induced coma’ in an intensive care unit. He concluded, almost laconically, that while in hospital he also contracted MRSA (a bacteria that’s more resistant to several widely-used antibiotics), pneumonia and septicaemia (blood poisoning). This is a demonstration of just how many diseases are nosocomial, and of how many so-called ‘cases’ of COVID-19 are in reality positive tests for SARS-CoV-2 of people who went to hospital for very different illnesses or injuries. Mr. Bainbridge’s Facebook post, which has subsequently been removed, didn’t say what he was ‘diagnosed’ with, but spinal taps are required to diagnose Guillain-Barré Syndrome (GBS), a neurological condition whose primary symptom is the ‘pins and needles’ he reported feeling, and which occurs when a trigger, such as a virus or a vaccine, mistakenly makes the immune system attack the nerves, causing pain and loss of co-ordination.
Undeterred, on 3 June Mr. Bainbridge posted another dig at ‘anti vaxxers’. This was the last post on his Facebook page; but alerted of the recording of his story on The COVID Blog, on 13 June he accused the blog of publishing ‘fake news’, claimed that the screengrabs of his Facebook page it had published were ‘out by over 10 years’, and threatened the author with ‘libel lawsuits’. Presumably, the success of such lawsuits will depend on Mr. Bainbridge establishing how he was posting about taking a COVID-19 ‘vaccine’ before 2011. Closer to the truth, in July this year, the US Food and Drugs Administration acknowledged that there was an increased risk of Guillain-Barré Syndrome from certain COVID-19 ‘vaccines’, including the AstraZeneca brand. Despite Mr. Bainbridge’s mockery of and contempt for the concerns and fears of millions of Britons, and his reckless promotion of an experimental drug programme, I wish him a quick and full recovery.
As a gesture to recording the effects of the drugs they have authorised for temporary use, the UK’s Medicines and Health products Regulatory Agency (MHRA) has what it calls a ‘Yellow Card’ scheme, through which those injected with a COVID-19 ‘vaccine’ can report adverse drug reactions, or ADRs. Until I started investigating these reactions, I had no idea the Yellow Card scheme existed, and I doubt most British citizens being injected with these ‘vaccines’ do either. And since, as we shall see, the MHRA attributes little if any diagnostic credibility to these reports, it is unclear what the purpose of filling out a Yellow Card is, other than to present a facade of accountability to the public on which these ‘vaccines’ are being experimented. However, as in so much about the medical consequences of the biosecurity state, whether that’s deaths resulting from lockdown restrictions or from the ‘vaccination’ programme, it’s on these official figures that we must rely to arrive at the truth they conceal.
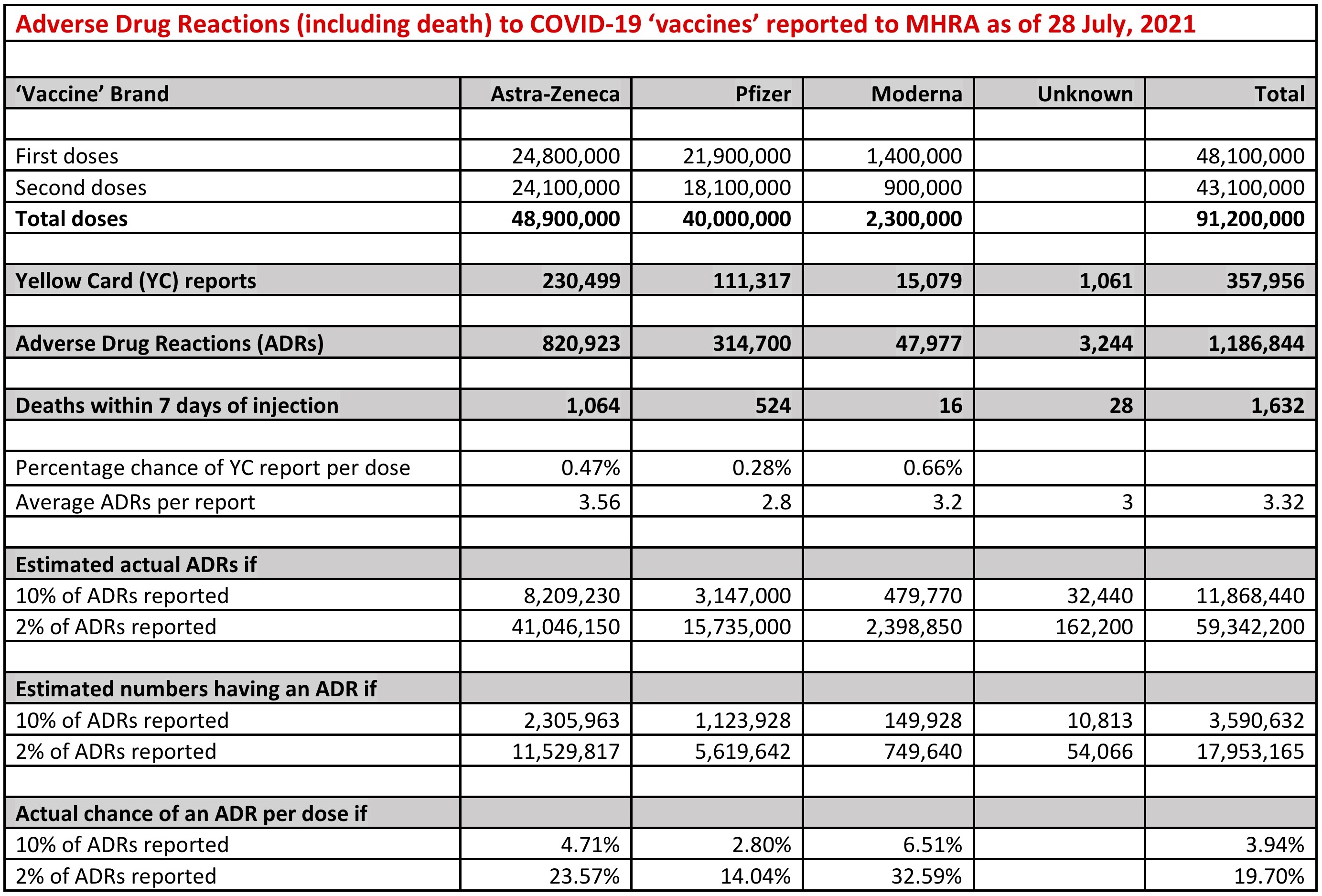
A summary of these Yellow Card reports is updated and published by the MHRA every Friday, and generally, in order to collate the figures, there’s about a week’ lag behind the received reports. I’m reporting here the most recent figures available at the time I finish writing this article. As of 1 September, 91.2 million doses of experimental, temporarily-authorised COVID-19 ‘vaccines’ have been injected into the UK public over a roughly 9-month period. This has resulted in 357,956 yellow-card reports to the MHRA of 1,186,844 adverse drug reactions (ADRs), including 1,632 deaths within 7 days of being injected. The number of reactions and deaths are not the same across the four brands of authorised ‘vaccines’, but vary considerably according to the pharmaceutical company producing and distributing the drug, which in the UK so far are limited to AstraZeneca, Pfizer and Moderna.
Adverse reactions to AstraZeneca’s Oxford-developed ‘vaccine’ include, but are not limited to: 7,407 blood disorders (of which 10 have been fatal); 9,214 cardiac disorders (162 fatal); 78,565 gastrointestinal disorders (14 fatal); 248,599 general disorders (358 fatal); 2,965 disorders of the immune system (4 fatal); 18,237 infections (92 fatal); 8,584 injuries (1 fatal); 8,631 metabolic disorders (3 fatal); 98,975 muscle and tissue disorders (1 fatal); 427 neoplasms (7 fatal); 174,814 disorders of the nervous system (191 fatal); 355 pregnancy conditions (6 fatal); 17,172 psychiatric disorders (5 fatal); 2,534 renal and urinary disorders (5 fatal); 17,023 reproductive and breast disorders; 27,616 respiratory disorders (129 fatal); 50,525 skin disorders; and 12,749 vascular disorders (66 fatal).
In total, after taking the viral vector AstraZeneca COVID-19 ‘vaccine’, there have been 820,923 adverse drug reactions, including 1,064 deaths within 7 days of injection, in 230,499 people from 48.9 million injections. That’s 1 or more (with an average of 3.56) ADRs in 0.47 per cent of those being injected.
Adverse reactions to Pfizer’s BioNTech-developed ‘vaccine’ include, but are not limited to: 10,736 blood disorders (of which 3 have been fatal); 5,129 cardiac disorders (95 fatal); 29,567 gastrointestinal disorders (14 fatal); 79,584 general disorders (180 fatal); 1,608 disorders of the immune system (2 fatal); 7,421 infections (81 fatal); 4,725 injuries (1 fatal); 1,760 metabolic disorders (1 fatal); 37,907 muscle and tissue disorders; 217 neoplasms (4 fatal); 55,002 disorders of the nervous system (51 fatal); 457 pregnancy conditions (16 fatal); 6,444 psychiatric disorders (1 fatal); 852 renal and urinary disorders (7 fatal); 18,171 reproductive and breast disorders (1 fatal); 13,500 respiratory disorders (49 fatal); 22,076 skin disorders (1 fatal); and 5,055 vascular disorders (13 fatal).
In total, after taking the messenger RNA Pfizer ‘vaccine’, there have been 314,700 adverse drug reactions, including 524 deaths within 7 days of injection, in 111,317 people, resulting from 40 million injections. That’s 1 or more (with an average of 2.8) ADRs in 0.28 per cent of those being injected.
Adverse reactions to Moderna’s ‘vaccine’ include: 1,895 blood disorders; 544 cardiac disorders; 3,860 gastrointestinal disorders; 13,877 general disorders (of which 8 have been fatal); 298 disorders of the immune system; 802 infections (2 fatal); 774 injuries; 250 metabolic disorders; 5,235 muscle and tissue disorders; 19 neoplasms; 7,473 disorders of the nervous system (1 fatal); 53 pregnancy conditions (2 fatal); 977 psychiatric disorders; 103 renal and urinary disorders; 2,388 reproductive and breast disorders; 1,253 respiratory disorders (1 fatal); 7,024 skin disorders (1 fatal); and 580 vascular disorders.
In total, after taking the messenger RNA Moderna ‘vaccine’, there have been 47,977 adverse reactions, including 16 deaths within 7 days of injection, in 15,079 people from 2.3 million injections. That’s 1 or more (with an average of 3.2) adverse reactions in 0.66 per cent of those being injected.
In addition to those recorded after taking the AstraZeneca, Pfizer and Moderna brands, there have been a total of 3,244 adverse drug reactions, including 28 deaths, in 1,061 people (an average of 3 ADRs) after being injected with an unspecified brand of COVID-19 ‘vaccine’.
However, concerning as the figures from the Yellow Card reports are, these are only the reported adverse drug reactions to the administered COVID-19 ‘vaccines’, which are well short of the actual number of ADRs and deaths following ‘vaccination’. We have to look elsewhere, but still to official estimates, to form our own estimates of the extent of the danger these drugs present to the health and lives of the British people. Fortunately, a year before the coronavirus crisis, in May 2019, the UK Government estimated that only 10 per cent of serious ADRs and between 2 per cent and 4 per cent of non-serious ADRs are reported to the MHRA. Unfortunately, in its Yellow Card reports, the MHRA doesn’t formally differentiate between serious and non-serious ADRs, but this increases the actual number of adverse drug reactions to the AstraZeneca ‘vaccine’ to between 8.2 million (with 10 per cent of ADRs having been reported) and 41 million (with 2 per cent of ADRs reported); to the Pfizer ‘vaccine’ to between 3.14 million and 15.73 million; and the total number of ADRs to COVID-19 ‘vaccines’ to between 11.87 million and 59.34 million. With an average of 3.56 (AstraZeneca), 2.8 (Pfizer), 3.2 (Moderna) and 3 (unknown) ADRs per report, this comes to between 3.6 million and 18 million people in the UK having suffered at least one adverse drug reaction from 91.2 million injections, or an ADR rate of between 4 per cent and 20 per cent of those injected. This is summarised in the chart below.
Despite these estimated figures, which are calculated from their own reports and estimates by the UK Government, in its summary of ‘Events with a fatal outcome’ the MHRA justifies the continued use of the COVID-19 ‘vaccines’ by dismissing even the reported deaths as ‘expected’, ‘natural’, and ‘mostly in the elderly’:
‘Older age and chronic underlying illnesses make it more likely that coincidental adverse events will occur, especially given the millions of people vaccinated. Several thousand deaths are expected to have occurred, naturally, within 7 days of the many millions of doses of vaccines administered so far, mostly in the elderly.’
Unfortunately, the MHRA provides no record of the age of the 1,632 people who have died within 7 days of an injection to substantiate this claim. But according to their report on the 72 people in the UK who have died from thromboembolic events (blood clots) with concurrent thrombocytopenia (low platelet counts) after being injected with the viral vector AstraZeneca ‘vaccine’: 7 were aged 18-29; 11 were 30-39; 12 were 40-49; 19 were 50-59; 9 were 60-69; 7 were 70-79; 3 were 80-89, 1 was 90-99, and 3 were of unknown age. So from this cause of death, at least, the MHRA’s claim that these were expected and natural deaths of the elderly is a misrepresentation.
Moreover, since the UK ‘vaccination’ programme began with the elderly and has now reached the 3.5 million children in the UK between 12 and 15 years old, we should have seen a reduction in the rate of deaths within 7 days of injection as the age of the ‘vaccinated’ lessened with the availability of the programme to younger and younger members of UK society. Instead, I have been collating these deaths roughly every fortnight for the past 6 months, and the number of deaths within 7 days has increased steadily with the number of injections, with 713 deaths as of 21 March; 847 deaths as of 5 April; 961 deaths as of 14 April; 1,213 deaths as of 19 May; 1,295 deaths as of 2 June; 1,328 deaths as of 9 June; 1,440 deaths as of 30 June; 1,536 deaths as of 28 July; 1,609 death as of 18 August; and 1,632 deaths as of 1 September. These figures don’t record the expected, natural and coincidental deaths of the elderly 7 days after ‘vaccination’, but rather the deaths across all ages of those ‘vaccinated’ with these experimental drugs.
The MHRA’s blanket dismissal of any causal connection between injection with a COVID-19 ‘vaccine’ and the 1,632 deaths within 7 days also doesn’t account for the different adverse drug reactions to the different brands of ‘vaccine’, with the AstraZeneca drug having a far higher number of ADRs per report (3.56) than Pfizer (2.8), and the chance of having at least one ADR per dose varying hugely between the brands, with people being injected with the AstraZeneca ‘vaccine’ having a 0.47 per cent chance per dose, compared with 0.28 per cent from Pfizer’s ‘vaccine’ and 0.66 per cent from Moderna’s. With the estimated number of actual ADRs, the discrepancies are even higher, with AstraZeneca ranging between 4.71 and 23.57 per cent per dose, Pfizer between 2.8 and 14.04 per cent, and Moderna between 6.51 and an extraordinary 32.59 per cent chance of an ADR per dose, almost 1 in 3. Given the huge numbers of doses administered, 91.2 million in the UK, we’d expect to see little if any difference between the ‘vaccines’ and the chance of an ADR if there were no causal connection between them. Instead, from 48.9 million doses of AstraZeneca’s viral vector ‘vaccine’ there have been 1,064 deaths within 7 days; while from Pfizer’s 40 million doses of mRNA ‘vaccine’ there have been 524, a huge difference unexplained by the natural deaths of people who coincidentally happened to have been injected 7 days before. From where do these differences in ADRs and deaths come, if not from the different contents of the COVID-19 ‘vaccines’? There has been some silent recognition of this, with only the Pfizer ‘vaccine’ authorised for children and the uptake on AstraZeneca almost halted as the consequences of being injected escape the censorship and lack of information available to the public. But no medical or legal accountability has been admitted, as if a handful of people had developed a nasty rash after being injected, rather than the 1,064 known deaths — and the many thousands more unreported or that occurred outside the MHRA’s arbitrary and medically-meaningless 7-day limit — that have fallen to AstraZeneca’s deadly drug.
It’s concerning, to say the least, that the Government body responsible for regulating medicines in the UK should dismiss deaths following injection with drugs whose clinical trials are incomplete, that employ bio-technology that has never been used on humans before, and that have only been granted temporary authorisation, as ‘coincidental’ and without causality. If there had been 90 million visits to, for example, UK hairdressers within 7 days of these deaths we would rightly dismiss any causal connection to what we could justifiably call a coincidence; but if there were 90 million visits to fast-food restaurants and 1,632 deaths of diners within 7 days, the British public would want to know which restaurants owned by McDonalds, Burger King or Kentucky Fried Chicken the dead ate at and what food they were served. Wouldn’t reports by 3.6 million restaurant diners of adverse reactions to the food, and over 18 million suspected adverse reactions, sending thousands of Britons of all ages to hospital, constitute sufficient plausibility to draw a causal connection between what’s being served and its effects? That the MHRA has no interest in either the restaurants or what they’re serving, continues to recommend both the restaurants and the food — and is, indeed, paid by the fast-food chain owners to do so — should be of more than concern to us. But then, that’s what happens when — to continue the analogy — the restaurant owners pay the Food Standards Agency to recommend their restaurants to a public instructed by the Government (on culinary advice from the same owners) that home cooking will kill you.
To drop the analogy with McDonalds, Burger King and KFC and return to the reality of AstraZeneca, Pfizer and Moderna, when up to 18 million British citizens have had an adverse drug reaction to the ‘vaccines’ of these pharmaceutical companies, and there is between 4 per cent and 20 per cent chance of having at least one, how is it that the MHRA can be so resolutely dismissive of the consequences of their temporary authorisation?
In its latest summary of the reports it has received, the MHRA claims that ‘over 133,079 people across the UK have died within 28 days of a positive test for coronavirus’. As we know, on the instructions of Public Health England, RT-PCR tests in the UK are used at a cycle threshold of 40, below which everything is deemed a ‘positive’. This means that traces of viral DNA amplified up to half a trillion times, at which only 3 per cent of positives are real, are recorded as a ‘case’ and identified as a ‘cause of death’. It’s on the basis of this grossly and deliberately manipulated calculation of the number of so-called ‘COVID-deaths’ that the MHRA argues that the ‘the expected benefits of the vaccines in preventing COVID-19 and serious complications associated with COVID-19 far outweigh any currently known side effects’. The MHRA concludes:
‘Review of individual reports and patterns of reporting does not suggest the vaccines played a role in these deaths. There are currently no indications of specific patterns or rates of reporting that would suggest the vaccine has played a role.’
Worrying as this denial of any causality is, though, it is not, unfortunately, surprising. Although an agency of the Department of Health and Social Care, the MHRA is entirely funded by the pharmaceutical industry it regulates, which includes AstraZeneca, Pfizer and Moderna, and which in 2013 was paying UK health professionals £40 million/year to promote their drugs. And as I have revealed in an earlier article, The Betrayal of the Clerks, over the past decade the MHRA has received £7.15 million from the Bill and Melinda Gates Foundation (BMGF), £1.37 million of it in 2020. In December 2017, the MHRA announced a partnership with the BMGF and the WHO worth £980,000, and both the current and former directors received funding directly from the BMGF. In September 2019, Dr. Ian Hudson left the MHRA to join the BMGF as Senior Advisor, Regulatory Affairs, Integrated Development, Global Health; and her successor, Dr. June Raine, claimed £5,035.69 in expenses to attend a BMGF meeting regarding the Smart Safety Surveillance (3S) project in Seattle, with the MHRA receiving a grant worth £292,000 from the BMGF in return. This is just a glimpse of the financial reality of how medicines, including the COVID-19 ‘vaccines’, are regulated under neoliberalism.
As a measure of the MHRA’s lack of transparency and honesty as a nominally public body funded by the industry and investors whose products it has the responsibility for authorising, in response to a Freedom of Information request made in February this year, asking what percentage of adverse reactions to COVID-19 ‘vaccines’ it estimates are being recorded by them, the MHRA simply refused to answer. Even under the orthodoxies of neoliberalism that over the past four decades have removed the barriers and checks to our transition into a biosecurity state, a Government agency that refuses an FOI request made under an Act of Parliament on the grounds of commercial confidentiality means that agency is not a public body but an arm of the pharmaceutical industry that funds it, and for whose business it competes with other regulatory agencies.
It was this financial dependency of regulator to client that contributed to the Grenfell Tower fire and the deaths of 72 people in June 2017, and continues to be a barrier to the ongoing scandal of hundreds of UK residential buildings, 4 years later, still clad in systems and materials that — whether or not they meet fire safety regulations — are a threat to the lives of millions of residents. The equivalent relationship between the MHRA and the immensely powerful pharmaceutical companies that fund it has already had far more serious and deadly consequences for those Britons injected with the COVID-19 ‘vaccines’ it has authorised for temporary use. And it’s not just the MHRA. The Department of Health and Social Care, Public Health England and the National Health Service also deny a causal connection between the ‘vaccines’ and all but a handful of the 1,632 deaths recorded within 7 days of injection.
We’ve already seen that these ‘vaccines’ neither prevent infection with SARS-CoV-2 nor lessen the severity of the symptoms of COVID-19; so to try and establish a more accurate comparison between the criteria by which a death is attributed to Coronavirus disease 2019 and a COVID-19 ‘vaccine’, on 12 April I sent a Freedom of Information request (below) to Public Health England, the National Health Service and the Office for National Statistics.
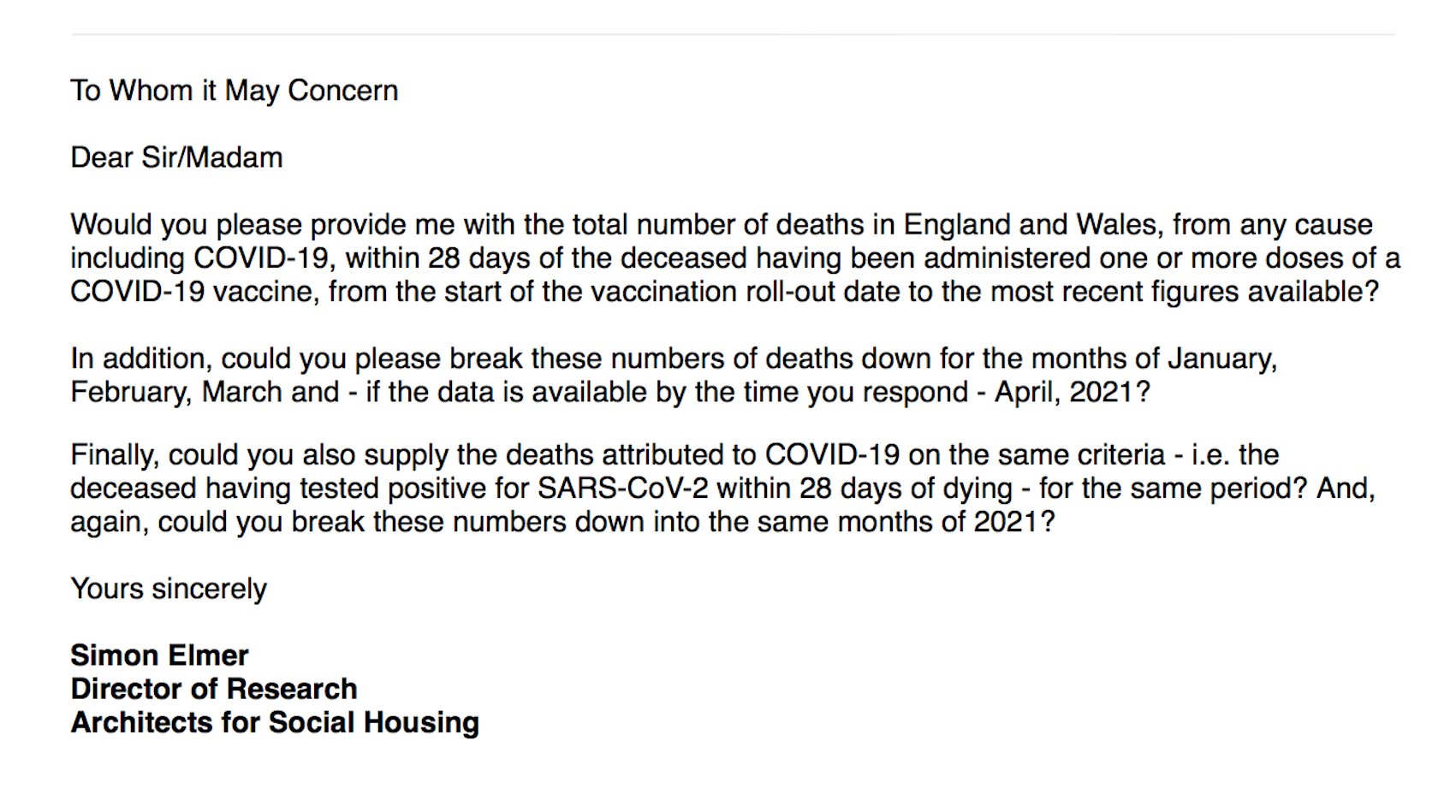
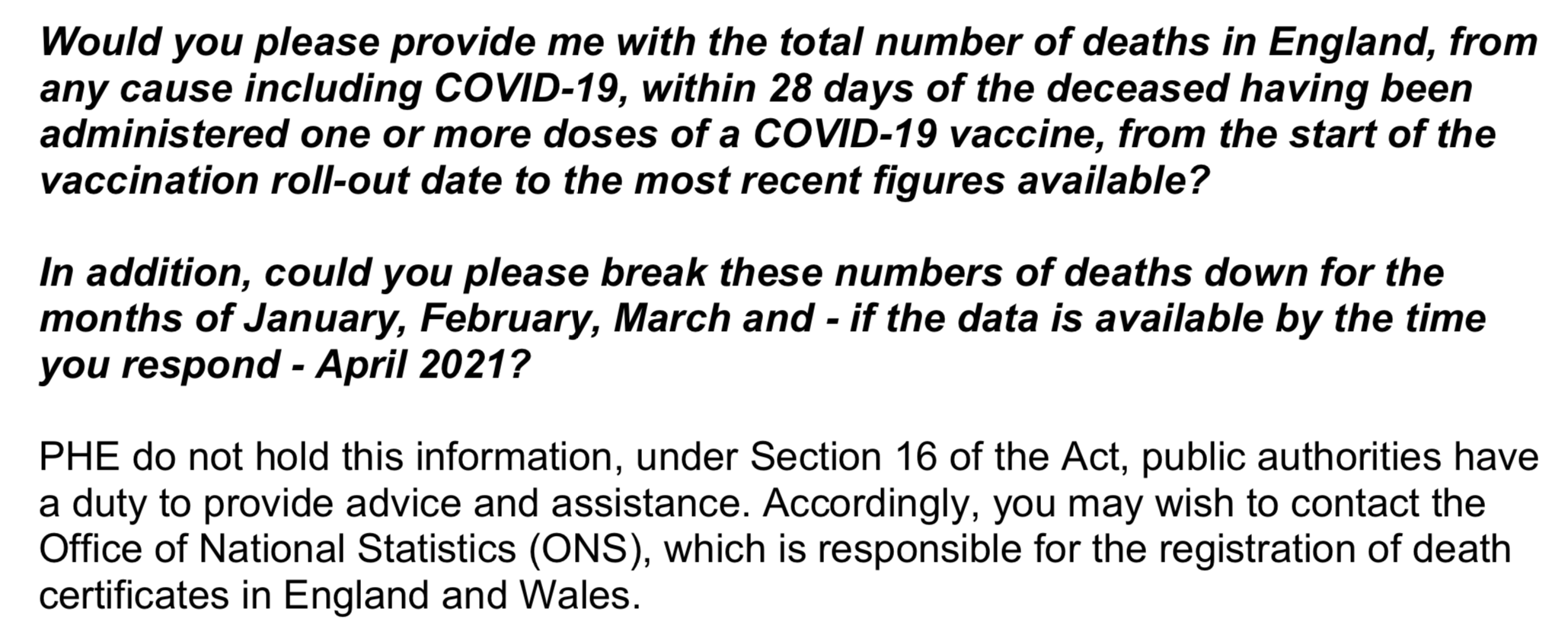
These are the organisations responsible for generating the completely fanciful and misleading figure of over 133,000 COVID-deaths with which the MHRA balances benefit to risk. But, despite the fact that all three publicise COVID-deaths on the criterion of a positive RT-PCR test within 28 days of death (in fact, even this is not required for a death be included in their calculations), all three responded that they do not record deaths within 28 days of taking a COVID-19 ‘vaccine’. This is the response from Public Health England, which I received 5 May, 2021:
This is the response from the Office for National Statistics, which I received on 7 May, 2021:
And this is the — very brief — response from the National Health Service, which I received by e-mail on 12 May, 2021:
It’s extraordinary enough that the three organisations responsible for calculating and publicising the number of so-called ‘COVID-deaths’ in England and Wales, and thereby for justifying to the public the lockdown restrictions enabling the implementation of the UK biosecurity state, do so by (among other criteria) counting deaths from any cause within 28 days of a positive result within a cycle threshold of amplification so high that it cannot identify either the virus or the cause of death. But that the same criterion isn’t applied by these same organisations to deaths from any cause within 28 days of receiving an experimental ‘vaccine’ they at least know the deceased was injected with is not extraordinary but sinister, and further calls into question their honesty and trustworthiness.
But to be honest myself, I never expected PHE, the ONS or NHS to release these statistics, because if they did, even the most ferociously devout of the COVID-faithful might be forced to confront the deliberate deception in the criteria for ‘COVID-deaths’ by which this so-called health crisis has been manufactured by these organisations. The fact is, depending on the time of year, around 10,000 people die every week in England and Wales at an average age of 80 for men and 82 for women. These, overwhelmingly, constitute the ‘COVID-dead’. Were the same criteria applied to those dying within 28 days of injection with a COVID-19 ‘vaccine’ applied to them, it would be surprising if the ‘vaccine-dead’ didn’t outstrip them.
As a comparison, though, this is not quite accurate. We would at least know that those deceased within 28 days of being injected did have at least one of the COVID ‘vaccines’ injected into their bodies; while there is nothing to show that an official ‘COVID-19’ death was infected with a sufficient dose of SARS-CoV-2 to be considered infectious, let alone for it to be a cause of COVID-19. According to this criterion, which has been misleadingly used to terrorise the people of the UK into participating in these experimental, unnecessary, dangerous and in many instances fatal medical interventions, the number of deaths within 28 days of injection would be even higher than the 1,632 recorded (but officially denied) deaths.
But whatever the actual number of deaths caused by the injection of these ‘vaccines’ — which have only been temporarily approved by the government arm of the pharmaceutical industry on the basis of an emergency that in reality never existed and even in its manufactured form disappeared long ago — we should be concerned about, and demand an answer to why they are employing, these double standards for falsely attributing deaths to COVID-19 and yet equally falsely dismissing deaths resulting from the UK ‘vaccination’ programme. Above all, we should be opposed to and resist the UK Government and its corporate partners in the global pharmaceutical industry making a programme of perpetual injection with these new biotechnologies a condition of our freedoms in the UK biosecurity state.
3. Deaths Following Injection with a COVID-19 ‘Vaccine’
On 21 May, 2021, Lisa Shaw, the previously healthy 44 year-old presenter for BBC Radio Newcastle, died of a brain haemorrhage. On 29 April, she has been injected with her first dose of a COVID-19 ‘vaccine’. This August, the Newcastle coroner, Karen Dilks, found the death to have been caused by ‘complications of an AstraZeneca COVID vaccine’, which she had ‘clearly established’ caused ‘thrombotic thrombocytopenia’ (blood clots) in Mrs. Shaw’s brain. Under Section 19 of the Coronavirus Act 2020, a doctor who has not seen the deceased is empowered to certify the cause of death (for example, as COVID-19) without the death being referred to the coroner before cremation of the deceased; so it is unclear why an autopsy was performed on Mrs. Shaw’s body. The most likely explanation is her relative fame, and the interest the UK press would take in the story should her family’s request for an autopsy be denied. Against the complaints of less famous families, tens of thousands of deaths have been misattributed to COVID-19 under this coronavirus-justified legislation, just as over 1,632 deaths within 7 days of injection and possibly thousands more within 28 days have been dismissed as coincidental by the MHRA. It’s important to bear in mind that the death of Mrs. Shaw occurred more than 3 weeks after injection, and that her death, therefore, like that of Rachel McKinney, will not be recorded by the MHRA.
But continuing the obfuscation with which these unrecorded deaths are shrouded and dismissed, the BBC article reporting Mrs. Shaw’s death stated that, according to the MHRA, there have been ‘332 reported cases and 58 reported deaths — after nearly 35 million doses of the AstraZeneca vaccine in the UK’. The BBC later updated this to ‘417 reported cases and 72 deaths’; but these figures only refer, respectively, to the reports of, and deaths resulting from, blood clotting (thromboembolic events), which is the only cause of death to which the MHRA admits any causality, and that exclusively with the AstraZeneca ‘vaccine’. In fact, the MHRA reports that, as of 18 August, when the BBC article was published, there had been 1,056 deaths within 7 days of receiving 48.7 million doses of the AstraZeneca jab, and 1,609 deaths in total. How many deaths there have been that occurred, like Lisa Shaw’s, within three weeks or more of injection with a COVID-19 ‘vaccine’ is what I’ll try to establish in this section.
The rejection of my Freedom of Information requests by Public Health England, the Office for National Statistics and the National Health Service was as far as I had got in trying to establish the level of risk and dangers to our health consequent upon being injected with a COVID-19 ‘vaccine’, when I was contacted by the Edinburgh Lothian & Borders Lockdown Sceptics. They told me that someone called Brendan O’Donnell — perhaps one of their members, I didn’t inquire — had had better luck than I in sending equivalent Freedom of Information requests to Public Health Scotland (PHS). In fact, I realised later that Mr. O’Donnell had shown me a response to an FOI he had received from PHS back in March about the number deaths that month within 28 days of a COVID-19 ‘vaccine’, and it was this that had first suggested to me sending the same FOI request to Public Health England, so the idea of doing so is his — or theirs. So high were the figures that the Lockdown Sceptics sent to me that I wrote to them requesting the corroborating evidence of their authenticity, which Brendan duly provided. So the research that has unearthed these figures is his, along with the credit for doing so, and it’s this I’m going to discuss in this section.
On 17 June, 2021, Mr. O’Donnell sent a Freedom of Information request to both the Scottish Government’s Directorate for COVID Public Health and Public Health Scotland, asking them to provide him with ‘the total numbers of deaths for any reason within 28 days of receiving a COVID-19 vaccine’ from the beginning of the ‘vaccine’ rollout in December 2020 up until 17 June 2021. The Directorate for COVID Public Health directed him to data published by Public Health Scotland on 23 June, and which covers the period from 8 December to 11 June. These show the ‘overall deaths from any cause that have occurred within 28 days of receiving a COVID-19 vaccine, broken down by date of death and vaccine type’, as follows: AstraZeneca, 3,643 deaths; Pfizer, 1,877 deaths; and Moderna, 2 deaths, making a total of 5,522 deaths.
The Directorate also recommended an analysis of the overall deaths also published by PHS on 23 June, in which it compares ‘the observed number of deaths to the expected number of deaths’, which appears on page 28-29 of the report, Public Health Scotland, COVID-19 Statistical Report: As at 21 June, 2021. PHS clarifies that their analysis ‘includes all recorded deaths due to any cause and does not refer to deaths caused by the vaccine itself.’ Since the ‘vaccination’ programme is being pushed on the entire adult population, they write:
‘Many people will experience an illness or death in the days following their vaccination by coincidence. This is particularly the case for those vaccinated early in the programme, when the programme prioritised the very elderly population and those with pre-existing underlying health conditions.’
As proof of which, PHS broke the deaths from all causes within 28 days of a COVID-19 ‘vaccine’ into age categories, with the following results. The tables below further divide the deceased into those who had one dose of a ‘vaccine’ and those who had two doses, but of the 5,522 persons who had died within one or two doses, 122 were under the age of 50; 951 were between the ages of 50 and 69; 1,349 were between 70 and 79; and 3,100 were over the age of 80. This means that 56 per cent of those dying within 28 days of a COVID-19 ‘vaccine’ were over 80; 80 per cent were over 70; and 98 per cent were over 50 years of age.

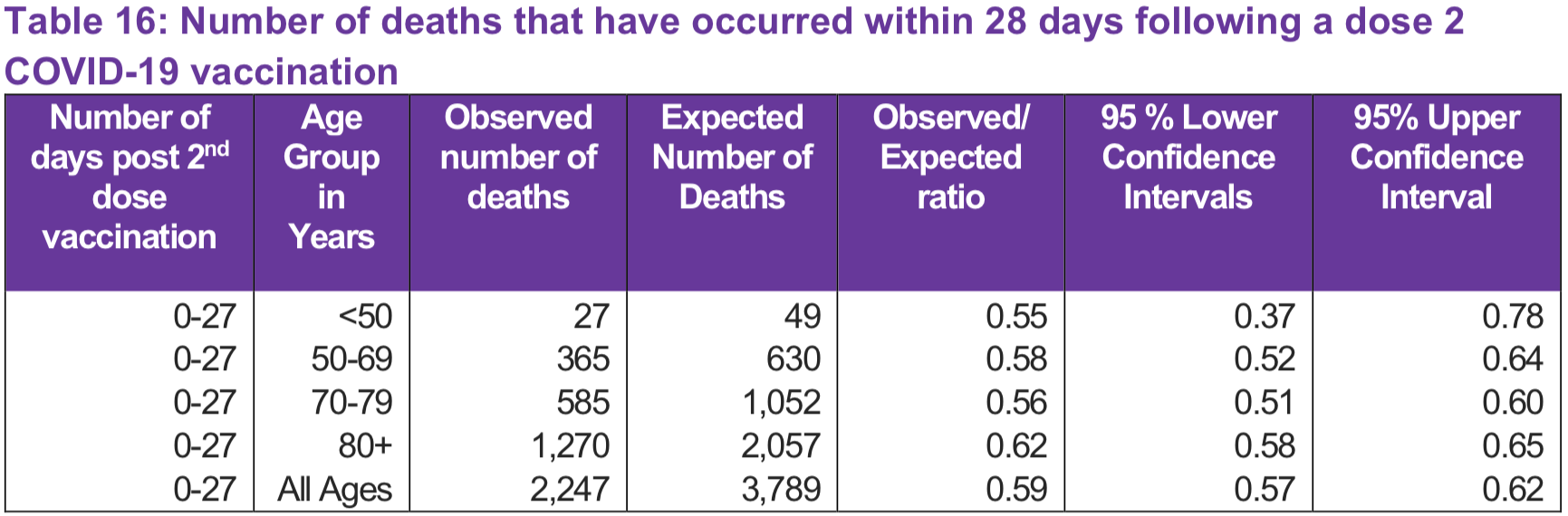
To substantiate this ‘coincidence’, PHS compared the total number of observed deaths within 28 days of a COVID-19 ‘vaccine’ with the ‘expected’ number of deaths among the vaccinated population. By ‘expected’ they mean ‘the average number of deaths that occurred per month (by age band and gender) for the same time-period between 2015 and 2019’. What this showed is that the 5,522 deaths between 8 December and 11 June was considerably less than the 8,718 expected deaths. To explain this lower rate of death (about 63 per cent of what was expected), PHS argues that, of the 6,358 excess deaths in Scotland between 16 March and 6 December, 2020, 5,363 were attributed to COVID-19, which therefore ‘may have caused premature deaths among some individuals prior to the start of the vaccination programme, who would have otherwise died in the months after the vaccination programme commenced.’ In other words, many of those whose deaths were attributed to COVID-19 in 2020 would have died anyway in 2021, whether or not they had the COVID-19 ‘vaccine’.
Finally, PHS also argues that, although high mortality rates in winter are ‘usually attributed to seasonal influenza’, in the winter of 2020-21 the rate of death from influenza in Scotland was ‘much lower than previous years’. They say this is ‘likely’ because of the lockdown restrictions in place to stop the spread of COVID-19 — although without explaining why such restrictions failed to save the 5,363 people whose deaths were attributed to this new airborne respiratory disease rather than influenza.
It’s difficult to comment on what PHS means by the ‘expected’ number of deaths, because they provide no information on how this has been calculated or about the ages of those expected to die. But if we look at the average number of deaths recorded by the National Records of Scotland (NRS) in the 26 weeks between 8 December and 11 June in the 4 years between 2016 and 2019, it comes to 30,592; so the 8,718 ‘expected’ deaths over the same time frame during the ‘vaccination’ programme constitutes 28.5 per cent of the total deaths, while the 5,522 deaths within 28 days of injection with a COVID-19 ‘vaccine’ constitute 18 per cent of the average number of deaths over the same period in the previous 4 years. That seems to me a large percentage to dismiss as expected within 28 days of ‘vaccination’; but the key thing to observe is that, with this figure, PHS is able to dismiss every one of the 5,522 deaths within 28 days of injection with these experimental ‘vaccines’ as a ‘coincidence’.
It’s curious, morover, that in explaining the deaths following injection with a COVID-19 ‘vaccine’ between 8 December, 2020, and 11 June, 2021, PHS refers to the deaths attributed to COVID-19 between 16 March and 6 December, 2020; because over the same 6-month period that the ‘vaccines’ were being administered in Scotland (specifically, between 7 December, 2020 and 7 June, 2021), according to the NRS, 4,033 deaths were attributed to COVID-19. Now, according to the World Health Organisation’s International Statistical Classification of Diseases and Related Health Problems followed by the NRS, a death from any cause must be attributed to ‘COVID-19’ if the disease is mentioned anywhere on the death certificate in accordance with the following classifications:
-
- Death within 28 days of a positive RT-PCR test (U07.1)
- Death where COVID-19 is ‘suspected’ (U07.2), and, from 22 March, 2021
- Death occurred after, rather than while, the deceased had COVID-19 (U09.9), and
- Death where a multisystem inflammatory syndrome has been ‘associated’ with COVID-19 (U10.9)
What’s curious about this is that, even according to these criteria for attributing a death to COVID-19, which rely on suspicions, associations and a testing regime denounced around the world as not fit for purpose, during the ‘vaccination’ programme in Scotland there have been 1,489 fewer deaths attributed to COVID-19 than have died within 28 days of receiving a COVID-19 ‘vaccine’. It seems reasonable, therefore, to subject the 4,033 deaths attributed to COVID-19 between 7 December, 2020 and 7 June, 2021, to the same analysis with which the 5,522 deaths following injection with a COVID-19 ‘vaccine’ have been dismissed by PHS as a ‘coincidence’.
Unhelpfully, the age categories used by the NRS are different from those used by PHS, but what their figures show is that, while 56 per cent of those dying within 28 days of a COVID-19 ‘vaccine’ were over 80 years of age, 80 per cent were over 70, and 98 per cent were over 50, of those whose deaths were attributed to COVID-19 according to the above criteria, 68 per cent were 75 and older, 87 per cent were 65 and older, and 99 per cent were 45 or older. So why, is the obvious question that no-one has answered, have these deaths of people of a similar age and in slightly fewer numbers over the same period of time not also been dismissed as a ‘coincidence’ and ‘expected’, rather than attributed to an unprecedented ‘pandemic’ justifying medically meaningless restrictions on our rights and freedoms?
The question becomes even more deserving of an answer when we look at the health of the deceased, not only over the past 6 months but throughout this so-called ‘pandemic’. According to the NRS’s latest report on ‘Deaths involving coronavirus (COVID-19) in Scotland’, in the 18 months between the week ending 16 March, 2020 (the date of the first official ‘COVID deaths’ recorded in Scotland) and 5 September, 2021, 10,612 people in Scotland had COVID-19 mentioned on their death certificate. Yet of the 10,396 who died up to 31 July, 2021, 93 per cent have been people with at least one pre-existing health condition, with 24 per cent having dementia or Alzheimer’s disease, 14 per cent having heart disease and 12 per cent with a chronic lower respiratory disease.

Moreover, of the 10,612 deaths attributed to COVID-19 in Scotland up until 5 September — the most recent date for which the NRS has published figures — 88 per cent were of people over 65 years of age, 71 per cent were over 75, and 39 per cent were 85 and over. Just 1 per cent, 106 people, were under 45 years old, with another 11 per cent, 1,146 people, between 45 and 64. To put this in the national context, in January 2021 the NRS reported that healthy life expectancy in Scotland is 61.7 years for men and 61.9 years for women. These are not figures that bear out the claims of a pandemic, but they do bear out accusations that the Scottish Government, with the collaboration of Public Health Scotland, has deliberately misled the public about the real level of threat from COVID-19.
And there is another question to be asked of PHS, as it should be of PHE. If the deaths from any cause within 28 days of injection are less than they expected, and there is, therefore, no reason to draw any causal link between any of those deaths and the various brands of COVID-19 ‘vaccines’, why are the other adverse drug reactions to those same ‘vaccines’ so much higher than other vaccines? As reported by The Exposé, on 29 May, 2021, someone called Duncan Husband sent a Freedom of Information request to the MHRA asking them to provide him with a list of all new vaccines in use in the UK between 2010 and 2020, along with the number of deaths, per vaccine, per month, within the same time frame. It isn’t stated explicitly in the FOI, but since the MHRA only records deaths within 7 days of injection, we must assume the same applies to these other vaccines.
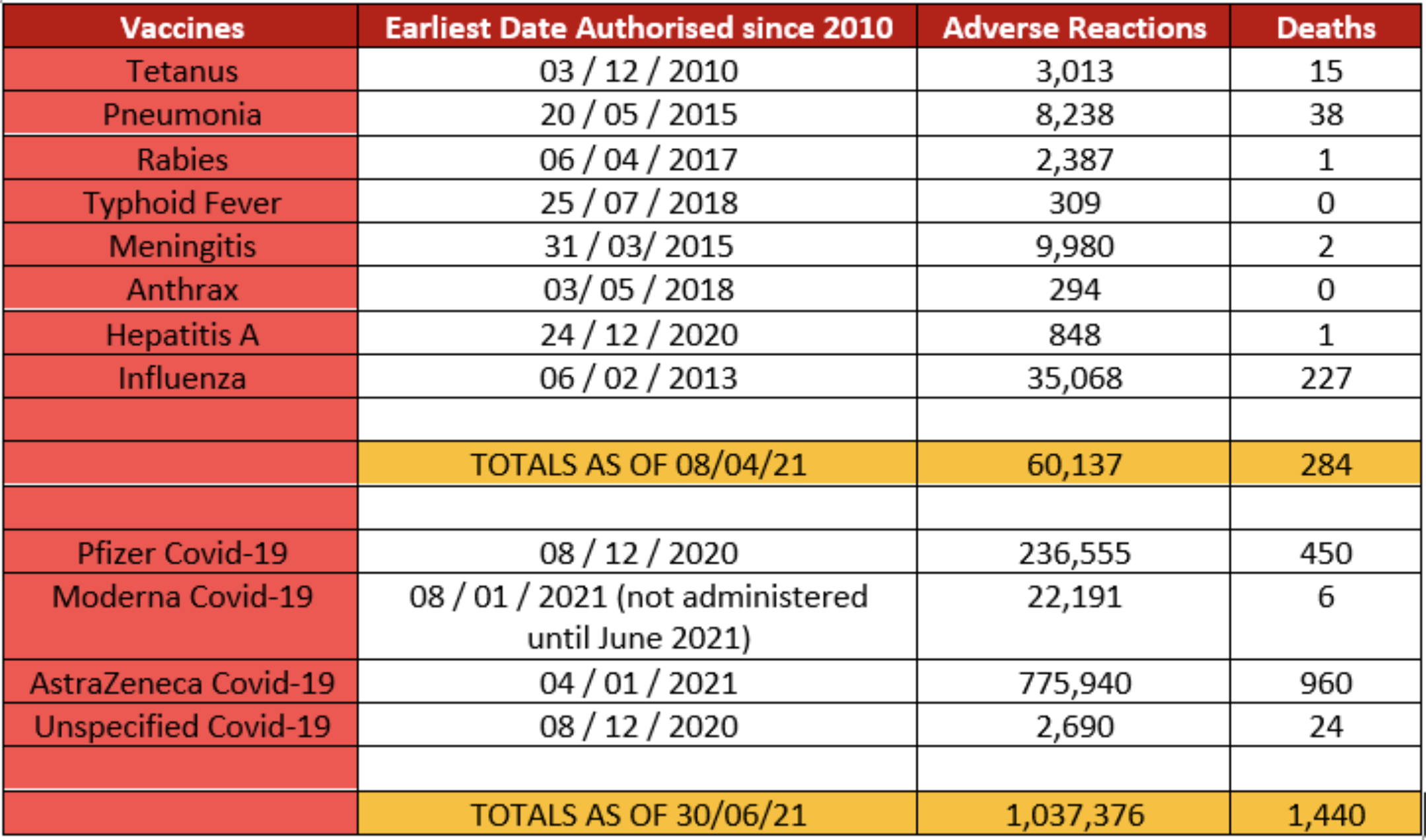
On 29 June, the MHRA responded with the information — although not broken down into each month — showing the total number of adverse drug reactions and deaths to the following vaccines:
-
- Pediacel, for diphtheria, tetanus and pertussis, which was granted authorisation by the MHRA in December 2010;
- Pneumococcal Polysaccharide, for pneumonia, authorised in May, 2015;
- Rabies vaccine, authorised in April, 2017;
- Vivotif, for typhoid, authorised in July, 2018;
- Menjugate, for meningitis, authorised in March 2015;
- Anthrax vaccine, authorised in May 2018;
- Hepatitis A vaccine, authorised in December 2020; and
- Influenza vaccines, the earliest of which was authorised in 2013.
What the MHRA’s figures showed is that, in total, as of April, 2021, these eight types of vaccines have resulted in 60,137 adverse drug reactions and 284 deaths. In comparison, as of 30 June, 2021, the most recent date for which figures were available before the article was published, there were 1,037,376 adverse drug reactions to COVID-19 ‘vaccines’ reported to the MHRA, including 1,440 deaths. This was, already, 17.25 times the 60,137 adverse drug reactions reported to the MHRA for all other vaccines approved in the UK since 2010.
Unfortunately, the MHRA didn’t provide the figures on how many doses of these other vaccines were administered since 2010, compared with the more than 90 million doses of COVID-19 ‘vaccines’ administered so far. But if both PHE and PHS can dismiss the deaths following injection with COVID-19 ‘vaccines’ as ‘natural’ deaths of people they expected to die anyway because of their age or pre-existing health conditions, how can they account for this enormous increase in the merely reported adverse drug reactions over such a short time when compared to earlier vaccines, no doubt each administered in smaller quantities but over a far longer period of time and for multiple infections and diseases? Is this, too, just a ‘coincidence’?
Finally, for the purposes of this analysis, the conclusion of Public Health Scotland, like that of Public Health England, that there is no causal relation between these ‘vaccines’ that have caused such a vastly increased number of adverse drug reactions and the thousands or even tens of thousands of deaths within, respectively, 7 days and 28 days of injection, are not shared by independent medical studies of the figures.
On 24 June, 2021, MDPI, the Multidisciplinary Digital Publishing Institute, published an article titled ‘The Safety of COVID-19 Vaccinations — We Should Rethink the Policy’. This was written by Dr. Harald Walach, professor at Poznan University of the Medical Sciences in Poznan, Pediatric Hospital, Poland and a visiting professor at Witten/Herdecke University’s Department of Psychology; Dr. Rainer J. Klement, a medical physicist with experience in data analysis and statistics based at the Radiation Oncology Department of Leopoldina Hospital in Schweinfurt, Germany; and Wouter Aukema, an Independent Data and Pattern Scientist in Hoenderloo, The Netherlands. From their analysis of the adverse drug reactions database of both the European Medicines Agency and the Dutch National Register, the authors concluded:
‘The COVID-19 vaccines have comparatively high rates of side effects and fatalities. The current figure is around four fatalities per 100,000 vaccinations, as documented by the most thorough European documentation system. Currently, our estimates show that we have to accept four fatal and 16 serious side effects per 100,000 vaccinations in order to save the lives of 2–11 individuals per 100,000 vaccinations, placing risks and benefits on the same order of magnitude. For three deaths prevented by vaccination we have to accept two inflicted by vaccination. This lack of clear benefit should cause governments to rethink their vaccination policy.’
This seems clear enough in its conclusion that these ‘vaccines’ are violating the medical principle to ‘first do no harm [primum non nocere]’. However, following an ‘expression of concern’ of undeclared origin about ‘misrepresentation of the COVID-19 vaccination efforts’, the MDPI editors — who one would have thought had checked the paper for the accuracy of its analysis before publishing it — initiated an investigation, and on 1 July the article was officially ‘retracted’. Their reasons for doing so, the editorial board wrote, was that the authors had drawn a causal relation between the reported adverse reactions, including deaths, and the COVID-19 ‘vaccines’; and the editors — like PHS and PHE — insisted that the ‘reporting of a death following vaccination does not imply that this is a vaccine-related event.’ They also note that the authors of the article were notified of the retraction ‘and did not agree’ with the decision. Once again, therefore, the vastly increased proportion of adverse drug reactions to the COVID-19 ‘vaccines’, including death within a week of injection, were dismissed by them as a mere coincidence. One has to wonder what the point of collecting this data is, if it can be so easily dismissed by those collecting it. Unfortunately, although this act of censorship of the only data we have recording the effects of these experimental ‘vaccines’ would, at any other time, be a cause for grave concern and investigation, under the European biosecurity state in which we now live it has become the norm.
To take a rather more open mind to the evidence of the figures published by Public Health Scotland, they appear to mean one of two things. Either:
-
- COVID-19 ‘vaccines’ are killing people in Scotland at a higher rate (870/month) then COVID-19 (670/month); or
- COVID-19 has had no impact on overall mortality, and the ‘pandemic’ is a creation of the criteria by which deaths have been attributed to it.
If they mean neither, and the deaths following ‘vaccination’ are all a coincidence, why have Public Health England, the National Health Service, the Office for National Statistics and the Medicines and Health products Regulatory Agency all refused to publish the figures on how many people have died in England and Wales within 28 days of a COVID-19 ‘vaccine’? The only answer to that I can suggest is that they would, almost undoubtedly, record a higher number of deaths per month than those dying within 28 days of a positive RT-PCR-test for SARS-CoV-2 and the other, wildly inaccurate, ways in which a death is attributed to COVID-19 in the UK and publicised by these organisations as a justification for lockdown restrictions, the ‘vaccination’ programme and biosecurity passports.
As chance would have it, on the same day I published this article, The Exposé revealed that a report published by the ONS on 13 September titled ‘Deaths involving COVID-19 by vaccination status, England: deaths occurring between 2 January and 2 July 2021’, in attempting to demonstrate the effectiveness of COVID-19 ‘vaccines’, inadvertently revealed (below) that over this 6-month period, there had been 14,265 deaths in England within 21 days of a first dose of a COVID-19 ‘vaccine’, and a further 11,470 deaths within 21 days of a second dose. That makes 25,735 deaths within 21 days of injection. If, as the Exposé does, we include the 4,388 deaths within 21 days of a first dose and 182 within a second dose that were categorised by the ONS as ‘involving’ COVID-19 (and we’ve seen how medically inaccurate this categorisation is), we get 30,305 deaths within 21 days of injection with a COVID-19 ‘vaccine’ over a 6-month period in England.

One might question why the ONS, in its reply to my FOI request, didn’t tell me that, although it doesn’t hold records of deaths within 28 days of injection with a COVID-19 ‘vaccine’, it does hold records of deaths within 21 days. But then, this is the sort of deliberate obstruction and half-lies with which all these organisations have concealed the consequences of the UK ‘vaccination’ programme from the British public.
As a thought experiment, therefore, I want to calculate what these unpublished figures might be, based on those published by Public Health Scotland. This calculation is only rough, because — as the average life-expectancy in Scotland compared to the UK shows — the health of the Scottish population is considerably poorer than in England and Wales. And with over 10,000 deaths in Scotland officially attributed to COVID-19 compared to the 133,000 in England and Wales, Scotland has a higher official COVID-19 death rate per capita than England and Wales. But in round numbers, Scotland, with a population in 2021 of 5.517 million, has 8.5 per cent the population of England (56.223 million), Wales (3.247 million) and Scotland combined (65 million). So, from the 5,522 deaths within 28 days of an injection with a COVID-19 ‘vaccine’ in Scotland between 8 December, 2020, and 11 June, 2021, we can calculate that, over the same period, around 54,000 people in England and Wales might have died within 28 days of injection with a COVID-19 ‘vaccine’. It’s now September, so we could add another 3 months of ‘vaccine’ deaths to that figure, increasing it by 50 per cent or more, as more of the population is ‘vaccinated’. Or we could extrapolate from the 30,305 deaths in the 6 months to 2 July to estimate the deaths within 21 days of injection over the past 2 months and arrive at over 4o,000 deaths in England alone. But let’s stop there. As I said, this is a thought experiment, but it gives us some idea of how many people might be dying as a result of the UK ‘vaccination’ programme, and why the medical bodies responsible for that programme have refused to make these figures known to the UK public.
It’s more likely, however, that the truth lies somewhere between a possible 97,000 ‘vaccine’ deaths in the UK and the 72 from blood clots to which the MHRA concedes some (‘extremely rare’) causality. As I have shown last year in my article, Manufacturing Consensus, in which I looked in detail at the criteria for attributing a death to COVID-19 and how this has produced the grossly exaggerated figures with which we continue to be inundated on a daily basis, the so-called ‘pandemic’ is — without a doubt — a product of the deliberately inaccurate methods and criteria for identifying and reporting a ‘COVID-19 death’. My own view is that the huge number of adverse drugs reactions (up to 1 in 5 injected) and unknown number of deaths from the ‘vaccines’ are a bi-product of the haste of development, inadequate trials, and experimental nature of the bio-technology they are deploying for the first time on human beings. These are, quite evidently, dirty drugs, pushed on a terrorised population by predatory pharmaceutical companies in collaboration with corrupt governments and unscrupulous medical advisors operating in a revolving door between both. But the aim of this global ‘vaccination’ programme, I believe — and it is, perhaps, no more than a belief, because the alternative is still unthinkable — isn’t mass murder, but the biosecurity passports that are the irreversible step into a totalitarian world.
As I also showed earlier this year, in Manufacturing the Crisis, what slight increase in overall mortality there has been in the UK — which last year, when adjusted for increase in both the size of the population and its age, had the 12th lowest mortality rate of every year since 1941 — has largely resulted (between half and three-quarters of deaths) from the withdrawal of medical care, treatment and diagnosis under the Government-imposed lockdown restrictions. However, all future deaths from coronavirus-justified medical interventions — which must now include COVID-19 ‘vaccines’ — and the withdrawal of medical care for other medical conditions under lockdown, will be attributed — as they have been up to now — to COVID-19. But statistically, as a cause of death comparable to heart disease, cancer, dementia and the other primary causes of death in the UK, COVID-19 does not represent any more of a threat to public health than seasonal influenza, and possibly considerably less. In no respect does it warrant the regulations and programmes of the UK biosecurity state. It certainly does not justify the mass UK ‘vaccination’ programme.
4. Overall Mortality in the UK Biosecurity State
On 14 March, Dom Busby, a 53-year-old BBC sports reporter, posted several photographs of himself on his Twitter account being injected with the Astra-Zeneca viral vector DNA ‘vaccine’, adding: ‘Well it didn’t hurt, now we just wait 15 mins and if you’re ok it’s off home. Please get this done!’ Five days later, on 19 March, he posted another photo of himself saying that he was back at work ‘after first ever days off through illness’. To accommodate what the UK Government claimed were delays in supplies of the ‘vaccines’ and the pharmaceutical companies claimed was a failure of capacity to administer them, the UK recommends a gap of 12 weeks between doses, so Mr. Busby would have been due to received his second injection on 6 June. Despite being a frequent user of Twitter, with 93 posts in March and 22 in early April, his final post was on 10 April. Two months later, on 10 June, the BBC reported that Dom Busby had died ‘after a short illness’.
No mention was made by the press of his ‘vaccination’ status; but in response to comments on his Twitter page, a friend and freelance broadcaster named Stuart Clarkson wrote that Busby had been receiving palliative care for several weeks and had finally died of an ‘inoperable brain tumour’. Clarkson was particularly incensed at those who dared to suggest that the ‘vaccine’ might have caused the tumour, writing a series of peremptory dismissals of such suggestions: ‘Please don’t use my friend’s death to fit your agenda when it doesn’t. Your dot-joining is flawed because you don’t know the facts. Goodbye.’ As to what these facts are, in April 2019 Dom Busby had posted a tweet about the death of the Scottish cricketer, Con de Lange, of a brain tumour at the age of 38; so it might be thought a little strange that he didn’t mention his own on his Twitter account. Perhaps he wanted the dignity of privacy which he didn’t apply to the public declaration and promotion of his own ‘vaccination’, but which I apologise, nonetheless, for violating here.
Let’s go back and look at the Office for National Statistics figures on registered weekly deaths in England and Wales in 2021. Since publishing Manufacturing the Crisis in January, I haven’t looked at these figures once, so I was as interested as I hope the reader is to see what the justification has been for keeping the UK under a third lockdown until 19 July, 2021.
In the first 29 weeks of 2021, ending 23 July — during which the UK had been under various tiers of biosecurity restrictions and the UK itself has officially been in an ‘emergency period’ that has continued beyond the lifting of those restrictions and which has been used to justify the authorisation of the experimental COVID-19 ‘vaccines’ — there was a total of 333,961 deaths registered in England and Wales. Of these deaths, 58,757 had COVID-19 mentioned on the death certificate under the same WHO categories used in Scotland: that is, a positive RT-PCR test within 28 days (U07.1), a suspected cause without a test (U07.2), death following COVID-19 but not with it (U09.9), or ‘multisystem inflammatory syndrome associated with COVID-19’ (U10.9). 33,674 of the deceased were over the age of 80; 46,901 were over the age of 70; 53,864 were over the age of 60 and 57,192 over the age of 50. Just 1,565 of the deceased were under 50 years of age. And for those in favour of ‘vaccinating’ the quarter of the population under 20 in the UK with these experimental and dangerous drugs, in 29 weeks a total of 22 children between 0 and 19 had their deaths attributed to COVID-19. What this means is that 57 per cent of official ‘COVID-deaths’ were over the age of 80; 80 per cent were over the age of 70; 92 per cent were over 60; and 97 per cent were over 50. The average life expectancy in the UK is just under 80 for a man and 83 for a woman. Deceased under the age of 50 whose deaths have been attributed to COVID-19 make up 2.7 per cent of the so-called ‘COVID dead’, or about the same percentage of positive RT-PCR tests for SARS-CoV-2 in the UK that are not false.
In fact, the figures are even worse than this. Of the 58,757 official deaths attributed to COVID-19, the ONS has recorded 51,243 in which COVID-19 was identified on the death certificate as the ‘underlying cause’. In comparison, in the first 29 weeks of 2021, the ONS has recorded 62,168 deaths in England and Wales in which influenza and/or pneumonia were mentioned on the death certificate, and 58,757 in which they were identified as the underlying cause. And, over the same period, there have been 109,181 deaths in which any respiratory disease other than COVID-19 has been mentioned on the death certificate, of which 27,521 have identified the respiratory disease as the underlying cause. If the same protocols for filling out death certificates were followed for so-called ‘COVID-deaths’, I have little doubt that a similar proportion of deaths would be more accurately attributed to the disease, and what we’d be looking at in 2021 is under 15,000 deaths in which COVID-19 had been identified as the underlying cause in people dying at the same age and in the same numbers as in any other year.
The only difference would be that, with the withdrawal of medical diagnosis, care and treatment for 68 million people under lockdown restrictions since March 2020, we have built up a vast backlog of premature deaths of the elderly and sick from cancer, heart disease, dementia, diabetes and the other health conditions responsible for overall deaths in the UK. As I’ve shown fairly conclusively, it is these neglected health conditions, and not a deadly new disease called COVID-19, that is responsible for the slight increase in deaths in 2021, as they largely were in 2020. The unavoidable fact, which the NHS, PHE, PHS and large swathes of the medical profession have been complicit in denying, is that if you drastically reduce medical care for a nation for 18 months, mortality rates will increase.
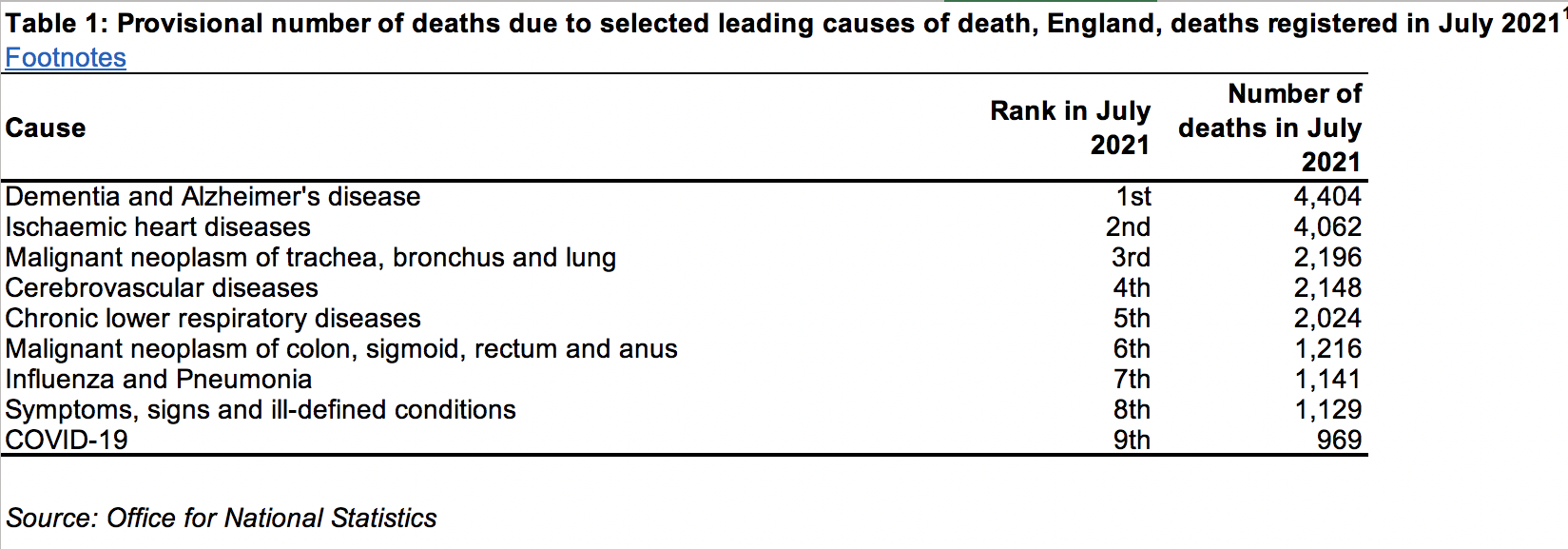
Until the ONS publishes the figures at the end of the year, I can’t repeat my previous analysis of these deaths by other causes; but as a cross section of where COVID-19 comes in the different causes of death — even according to the deliberately exaggerated number of deaths attributed to the disease — according to a series of FOI requests (now the only way, it seems, to extract truth out of the institutions repeatedly and consistently lying to the British people), in July 2021, the 969 deaths attributed to COVID-19 constituted the 9th leading cause of death in England, with dementia and Alzheimer’s disease first with 4,404 deaths, followed by ischaemic heart diseases in second with 4,062, and malignant neoplasms (cancers) of the trachea, bronchus and lung in third with 2,196, as follows:
In June 2021, the 344 deaths attributed to COVID-19 constituted the 26th leading cause of death in England, far behind, once again, 4,183 deaths from heart diseases, 3,962 deaths from dementia and Alzheimer’s disease, and 2,241 deaths from neoplasms.
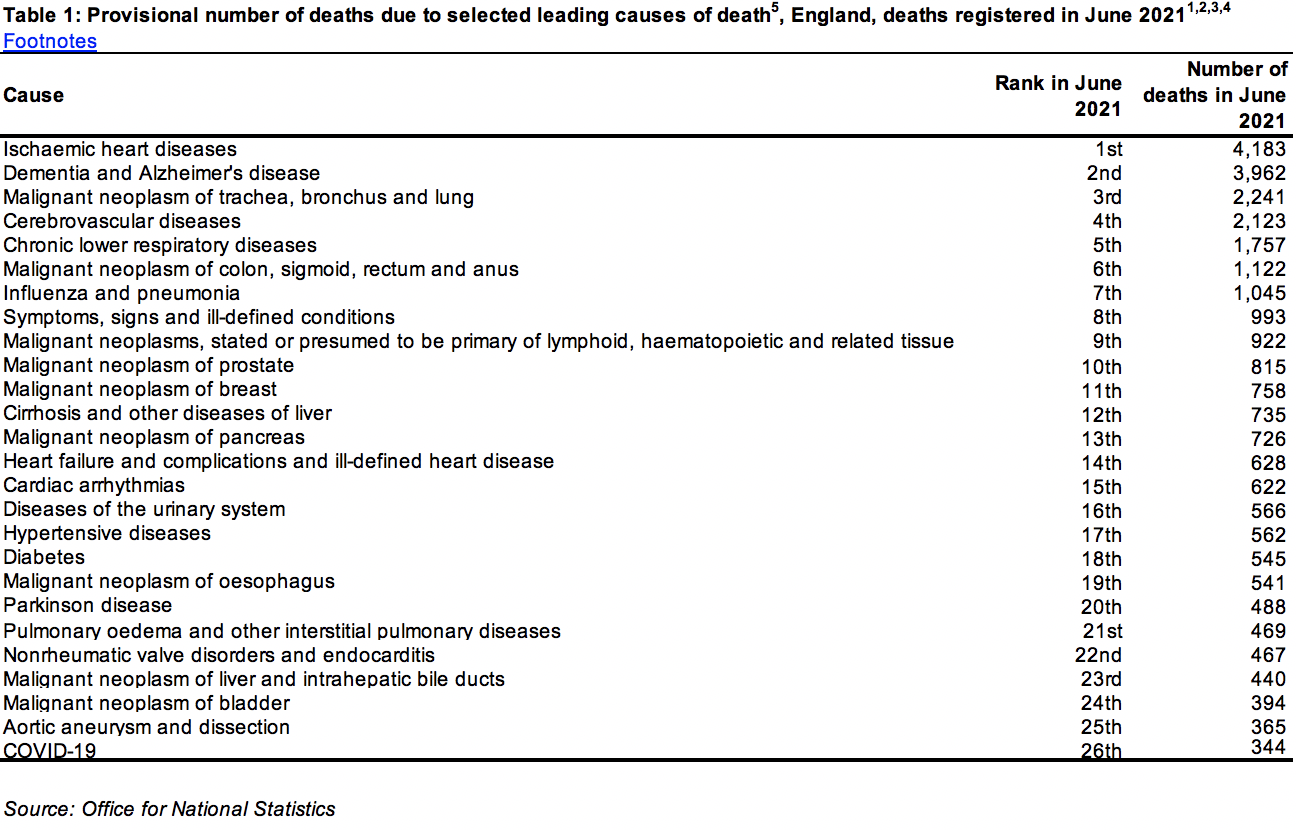
While in May, 2021, the 333 deaths attributed to COVID-19 constituted the 24th leading cause of death in England, after 3,780 deaths from heart disease, 3,711 from dementia and Alzheimer’s, 2,011 from neoplasms.
Why is it that the medical advisors to the Government, the heads and representatives of the NHS, the worried doctors and exhausted nurses wheeled out to encourage, bully and threaten us every day to be injected with a COVID-19 ‘vaccine’, show no concern with how restrictions on visits to care homes, the imminent banning of thousands of care-home staff who are not ‘vaccinated’, the unrelenting fearmongering from the Government and media about the grossly exaggerated and wildly inaccurate threat of COVID-19, the increased anxiety among the elderly, vulnerable and young caused by 18 months of social distancing and mask wearing, the compromise of our immune systems caused by being shut up indoors for months on end, and all the other lockdown restrictions are taking their toll on the health and lives of the British people? Why is it that — supposedly in order to contain a disease that ranked below diseases of the urinary system and non-rheumatic valve disorders in the causes of death this spring, and below influenza and pneumonia this summer — the UK has been kept under lockdown restrictions whose only impact on the health of the public has been a negative one?
It is no surprise that the 384,936 deaths in England and Wales in the first 35 weeks of 2021 (ending 3 September, the most recent figures) are over 22,000 more than the 362,754 annual deaths on average in the same weeks between 2015 and 2019, when mortality rates in the UK were at the lowest they’ve been since records began in 1941. Unfortunately, although we know that the age-standardised mortality rate in 2020 (1,043.5 deaths per 100,000 of the UK population) was surpassed in 2008 (1,091.9 deaths per 100,000) and every previous year back to when records began in 1941, I am not able to calculate the most recent year in which deaths in the first 35 weeks surpassed those in 2021, because the ONS breakdown of the weekly data on mortality only goes back to 2010.
What we do know, however, is that if the UK Government, its medical advisors and the heads of the National Health Service pursue policies which — whether intentionally or through criminal neglect — must inevitably result in the deaths of those who have been, and continue to be, denied medical diagnosis, treatment and care, while at the same time subjecting them, under the name of lockdown ‘measures’, to direct or consequential attacks on their physical and mental health — the most deadly of which, perhaps, is the ‘vaccination’ programme itself — the number of deaths among the elderly, those with pre-existing medical conditions, and those who have been ‘vaccinated’ will increase — but it’s not because of COVID-19. On the contrary, this is the consequence of our disastrous and duplicitous response to a virus and a disease that presents no threat to the public health of the nation.
So how is it, then, that the UK ‘vaccination’ programme has reached a stage of public compliance that it is on the cusp of being made a condition of UK citizenship, is about to be imposed on British children as young as 12 years old, and one day may be made compulsory for us all? How can we begin to explain this mass conversion to the new virtues of biosecurity? These are some of the questions I’ll address in the second part of this article, whose table of contents is as follows:
Part 2. Virtue and Terror
-
- Censorship and Consent
- How to ‘Vaccinate’ UK Children
- Virtue and Terror
- Crime and Punishment
Simon Elmer
Architects for Social Housing
Collections of writings by the same author about the UK biosecurity state :
Brave New World: Expanding the UK Biosecurity State through the Winter of 2020-2021
COVID-19: Implementing the UK Biosecurity State
Architects for Social Housing is a Community Interest Company (no. 10383452). Although we occasionally receive minimal fees for our design work, the majority of what we do is unpaid and we have no source of public funding. If you would like to support our work financially, including the research for these articles, please make a donation through PayPal:
![]()

It looks like deaths within 21 days of a vaccination ARE being collated. Further info here: https://theexpose.uk/2021/09/15/30k-people-died-within-21-days-of-having-a-covid-19-vaccine-in-england/
LikeLike
That is interesting. Thank you for letting me know, Jon. I’ve now added this information to the article.
LikeLike
Excellent and compelling, as always. Thanks for your stellar work.
Awaiting Part II with eager anticipation.
LikeLike
Hello E., you might be interested in my new book, The Road to Fascism: For a Critique of the Global Biosecurity State, which I’ve been working on since February this year and published today. It’s available as a print-on-demand book in hardback and paperback editions (with an e-book forthcoming). Please click on this link for the contents page, my preface and purchase options. Best wishes. https://architectsforsocialhousing.co.uk/2022/09/28/the-road-to-fascism-for-a-critique-of-the-global-biosecurity-state/
LikeLike
Brilliant piece. I live in Gibraltar which went from having the lowest death rate in the world to the highest within 10 days of the vaccination program starting. Those who died were in the care homes many given no choice whether they received it or not. So horrendous there was supposed to be an inquiry but it has been brushed under the carpet and now Gibraltar is going ahead with vaccinating 12 – 15 year olds.
LikeLike
Hello Elaine, you might be interested in my new book, The Road to Fascism: For a Critique of the Global Biosecurity State, which I’ve been working on since February this year and published today. It’s available as a print-on-demand book in hardback and paperback editions (with an e-book forthcoming). Please click on this link for the contents page, my preface and purchase options. Best wishes. https://architectsforsocialhousing.co.uk/2022/09/28/the-road-to-fascism-for-a-critique-of-the-global-biosecurity-state/
LikeLike
You say: “…since 1 February… of the 1,091 people who died after two injections, 1,054 were 50 years of age or older (97 per cent), while of the 536 who died without being ‘vaccinated’, 437 were 50 or over (81.5 per cent).”
Maybe I haven’t understood correctly, but surely this means that of those who died after 2 injections, 37 were under 50 and amongst the unvaccinated 99 were under 50. Now, I agree that the vaccine has to be examined very critically (I myself will not get vaccinated unless it’s either that or they put me in a camp for the unvaccinated, with “Vaccines Macht Frei” over the gate) but this implies that to a certain extent the vaccine protects you (I’ve seen statistics showing the vaccine is only 42% effective, which apparently counters the WHO’s rule that for a vaccine to be considered reliable it has to be over 50% effective).
Please explain.
LikeLike
Hello Sam. Thank you for your question. As I write in the text, I was quoting these figures to show that the figures published by the PHE showing 1,798 deceased who were diagnosed with the Delta variant having been ‘vaccinated’ at least once compared to 536 who hadn’t been injected can’t be dismissed, as they have been on social media, as more elderly people having been ‘vaccinated’ and therefore more are expected to die. The ‘vaccinated’ dead are slightly older than the ‘unvaccinated’ by the percentages I’ve calculated. But yes, you’re also right that the figures also mean, in flat numbers, that 99 ‘unvaccinated’ hospital patients diagnosed with the Delta variant died who were under 50, compared to 37 ‘vaccinated’ patients. If you want to interpret a difference of 62 deaths in 7 months in a population of 56 million that have been attributed to COVID-19 by the continued use of an RT-PCR test used at 40 Ct or one of the other three categories of ‘COVID-19 death’ and then later diagnosed as infected with the Delta variant as sufficient proof of the effectiveness of COVID-19 ‘vaccines’, you can, but I don’t think that constitutes anything like sufficient evidence.
As I make reference to throughout this text, as I do in the others I’ve written, the data published by PHE, the NHS, ONS and MHRA is so corrupted by the criteria by which it has been produced that it’s very hard to make any judgement about what is happening. But that in itself should be indicative, if not necessarily evidence, of deliberate deception and wrong-doing. But unfortunately, it’s all we have to go on. What I try to do is knock competing data against itself, as it were, and see what explanation of the outcome is the most rational. You’ve compared two figures from the first section of my article, which I don’t think justify the conclusion you propose. There are a lot more figures in the rest of the article about the effects of these ‘vaccines’. If you still think they protect us, or even maybe just the young, when you’ve finished, come back to me and we’ll talk some more. Best wishes.
LikeLike
I don’t think that they protect us. Nor do I say they do – I merely pointed out a slight contradiction in your argument. Even the official discourse (in France, at least, which is where I live) a few weeks ago was that it’s only 42% effective, as I’ve already said. So, at best they hardly protect us even according to the State.
If you look at the entry for today (17/9/21) on my site – https://dialectical-delinquents.com/covid1984-latest/2021-2/september-2021-covid1984/ – you’ll see some statistics from Israel showing how inefficient the vaccine is.
There are some other things in your article which I’m wary of, but I’ll leave it at that for the moment.
P.S.
Can I “advertise” an article I wrote back in May – “Conspirouettes” – https://dialectical-delinquents.com/conspirouettes/ ? It criticises the dogmatic anti-conspiracy theory ideologies as much as the conspiracy theories.
LikeLike
I think the absolute risk reduction figures (rather than the relative risk reduction figures that the vaccine manufacturers quoted for “effectiveness”) were somewhere ariund the 1% mark. Almost non existent!
LikeLike
Yes, according to a study published in the Lancet, the absolute risk reduction, which is the difference between attack rates with and without a ‘vaccine’, is 0.84% for Pfizer’s messenger RNA ‘vaccine’, 1.2% for Moderna’s mRNA ‘vaccine’, and 1.3% for AstraZeneca’s viral vector ‘vaccine’. This has cost the UK over £13 billion, the bulk of it going into the pockets of these pharmaceutical companies. A fool and his money are easily parted, and this generation are the biggest fools in British history.
LikeLike
For the last six months, up to week ending September 3rd, ONS data England & Wales total deaths are 1% below the five-year average of 2015-9. So its just normal – no excess. For week ending 3rd September there was a mere 6% excess of total deaths.
But back in January-February there was a large excess of mortality, probably due to government terrorising the people with lockdown plus ‘dark winter’ fears.
So I’m really puzzled by this – I thought the ‘vaccine’ was killing a lot of people, but if these ONS stats are reliable its not showing up.
LikeLike
Hello Nick, you might be interested in my new book, The Road to Fascism: For a Critique of the Global Biosecurity State, which I’ve been working on since February this year and published today. It’s available as a print-on-demand book in hardback and paperback editions (with an e-book forthcoming). Please click on this link for the contents page, my preface and purchase options. Best wishes. https://architectsforsocialhousing.co.uk/2022/09/28/the-road-to-fascism-for-a-critique-of-the-global-biosecurity-state/
LikeLike
This video from Israel might interest you:
https://www.vaxtestimonies.org/en/
LikeLike
Thank you for this. I’m puzzled by a particular feature of the PHE table you reproduce near the end of the first section of your article (which unfortunately doesn’t copy into this comment box). The Epose has used the same PHE table as you have and made similar points in its piece “13 reasons why you should not allow your child to get the Covid-19 Vaccine” published on 14 September and I’m asking them the same question I’m putting to you.
In this table of ‘Attendance to emergency care and deaths…Delta variant…by vaccination status 1 February-29 August’ there are 4 categories of people: those up to 21 days post first dose, those beyond 21 days post first dose, those beyond 14 days of a second dose, and unvaccinated. The only explanation I can think of for omitting those within 14 days of a second dose is that you are not officially considered to be vaccinated at all until 14 days have elapsed and the attendances at emergency care/deaths of those people are, presumably, included in the ‘unvaccinated’ column. The corollary would be that the figures for those demarcated by the 21-day cut-off for the first dose only represent those people attending/dying from 14 to 21 days after vaccination and, again, the 0-14 day cohort is subsumed in the ‘unvaccinated’ column.
If I have got this right the figures for attendances and deaths with the ‘Delta variant’ among the unvaccinated have been inflated by an unknowable number and, of course, correspondingly reduced for the actually vaccinated. In which case, yet again, you really have to hand it to them don’t you?
What do you reckon?
LikeLike
Interesting question, Alan. You’re right that the PHE data doesn’t include the number of patients who have attended emergency care in less than 14 days since their second injection of a COVID-19 ‘vaccine’. However, since they must have had their first injection, I’d guess they would be included in the 21 days or more since the first injection, rather than among the ‘unvaccinated’. From what I understand, the term ‘fully vaccinated’ is used to refer to those who are still alive 14 days or more after receiving their second injection, even if they have a positive RT-PCR test for SARS-CoV-2 or have developed symptoms of COVID-19, as so many of them have. But you’re right, the term ‘unvaccinated’ is confusing, particularly since neither the messenger RNA nor the viral vector injections are vaccines in the way we understood the term before the biosecurity state started rewriting the dictionary of medical practice.
LikeLike
Thank you for your reply. Yes, fair enough, as you suggest, the ‘0-14 day 2nd.-jabbed’ will be in the ‘post 21 day1st.-jabbed’. (I may have got a bit carried away there…) However, that still leaves open the question of the 0-14 day1st.-jabbed (does the 14-day wait apply to the first one?) and I’m wondering why PHE has used a 21 day cut-off, to create separate categories for those 1st.-jabbed, at all – if not to obscure this issue….
As you’ve written, we can expect the official data to be corrupted by the criteria by which it is produced. I’m hoping not to be merely setting hares running but my default attitude to all official data/pronouncements now is sceptical, if not cynical! .
LikeLike
Stop press! The latest version of the data in question has ‘1-21 days post 1st. dose’ as the column heading, thereby finishing the job of demolishing my little theory. I’ll get me coat.
LikeLike
Hello Alan, you might be interested in my new book, The Road to Fascism: For a Critique of the Global Biosecurity State, which I’ve been working on since February this year and published today. It’s available as a print-on-demand book in hardback and paperback editions (with an e-book forthcoming). Please click on this link for the contents page, my preface and purchase options. Best wishes. https://architectsforsocialhousing.co.uk/2022/09/28/the-road-to-fascism-for-a-critique-of-the-global-biosecurity-state/
LikeLike