‘Give them bread and circuses and they will never revolt.’ — Juvenal
Over the past week the race for a vaccine for COVID-19 has approached the finishing line, with the Oxford Vaccine Group looking to be the first to cross in the UK. This has occasioned a huge and relentless promotional campaign by the Department of Health and Social Care. In doing so, it has drawn on three media-friendly figures, in particular, to guarantee the safety of the vaccine: Dr. June Raine, Professor Andrew Pollard and Professor Jonathan Van Tam. The latter became a social media hit earlier this month after he compared the public’s adherence to Government lockdown restrictions to footballers holding their nerve for a ‘penalty shootout’; and likened the arrival of the COVID-19 vaccine to a ‘train coming round the bend’, with ‘the guard making sure it’s safe to open the doors’ equated to the Medicine and Healthcare products Regulatory Agency. This, it turns out, is the way to speak to a terrorised and infantilised British public; but if I can attempt something a little less metaphorical and address myself instead to thinking adults, here is a brief resume of these three figures about whom the British public should know something before boarding this particular train.
1. Doctor June Raine
Dr. June Raine is the Interim Chief Executive Officer of the Medicines and Healthcare products Regulatory Agency (MHRA) responsible for overseeing the safety of medicines used in the UK, including the COVID-19 vaccine. Despite its status as a executive agency of the Department of Health and Social Care, over the past decade the MHRA has received $7.15 million from the Bill & Melinda Gates Foundation (BMGF), which in June this year invested $1.6 billion in GAVI, the Global Alliance for Vaccines and Immunisation. Ten years ago in January 2010, the BMGF invested $10 billion in vaccine production as part of its call for a ‘Decade of Vaccines’. However, Dr. June Raine’s association with the Bill & Melinda Gates Foundation is more than financial. In March 2015, she attended a lecture on ‘Global health changes and overcoming regulatory challenges’ delivered by Dr. Dan Hartman, Director of Integrated Development for the BMGF, at the tenth MHRA Annual Lecture. 6 months later, in September 2015, at a forum on ‘Real world evidence’ held by the Academy of Medical Sciences and the Association of the British Pharmaceutical Industry, Dr. Raine stated that, as regulation becomes increasingly proactive in planning active surveillance, ‘the world of reactive regulation is the world of the past’.
In 2019, Dr. Raine claimed £5,035.69 in expenses to attend a BMGF meeting regarding the Smart Safety Surveillance (3S) project in Seattle. In the same year, the MHRA received a grant worth £292,000 from the Bill & Melinda Gates Foundation. Two years before that, in 2017, Dr. Raine’s predecessor as Chief Executive Officer of the MHRA, Dr. Ian Hudson, received £980,000 from the BMGF, before leaving in September 2019 to join the Foundation as Senior Advisor, Regulatory Affairs, Integrated Development, Global Health. The Office of the Advisory Committee on Business Appointments found ‘no particular risk of impropriety’ in this revolving door between a senior civil servant in a regulatory government agency funded by global investors in vaccines and a full-time, paid role in with the same investors.
2. Professor Andrew Pollard
This conflict of interest between producer and regulator is also present in the many roles of Professor Andrew Pollard, who is both Director of the Oxford Vaccine Group producing the COVID-19 vaccine in partnership with the British-Swedish pharmaceutical company AstraZeneca, and at the same time a member of the National Institute for Biological Standards and Control (NIBSC) Scientific Advisory Committee, which advises the Medicines and Healthcare products Regulatory Agency (MHRA) that guarantees the safety of vaccines in the UK. The Chair of the NIBC Committee, Professor David J. Webb, is an MHRA Board Member.
Dr. Pollard’s employer, the University of Oxford, where he is Professor of Paediatric Infection and Immunity, has received $11.64 million for vaccine development from the Bill & Melinda Gates Foundation over the past 3 years, and $208 million in grants over the past decade. In 2016, the BMGF gave $36.9 million for research into vaccine development by a team that included the Oxford Vaccine Group, which was headed by Professor Pollard. In addition, Professor Pollard’s own Laboratory is also funded by the Bill and Melinda Gates Foundation.
As Director of the Oxford Vaccine Group, which in 2013 affiliated with the newly-created agency Public Health England, which itself has received $7.46 million in grants from the BMGF, Professor Pollard developed the Meningitis B vaccine Bexsero. Under pressure from the Secretary of State for Health, who at the time was Jeremy Hunt, following his appointment that same year as Chair of the Joint Committee on Vaccination and Immunisation (JCVI), Professor Pollard mandated the use of Bexsero for UK children, despite significant safety signals for Kawasaki Disease and the rarity of Group B meningococcal disease. There were 5 cases of Kawasaki Disease in 4,340 trial infants, and more than one-third of infants had high fever the day of vaccination, including 8 who had seizures.
In 2015, production of the vaccine was taken over by GlaxoSmithKline (GSK), the British pharmaceutical company that in 2009 had developed the Pandemrix vaccine in response to the threat of swine flu, which was predicted to kill 65,000 people in the UK. In September 2010, an article published in the Journal of the American Medical Association showed that the risk of serious illness resulting from swine flu was no higher than that from seasonal influenza, and in actuality, swine flu killed 457 people in the UK. The ‘independent’ modeller who made these predictions was none other than Professor Neil Ferguson of Imperial College London, who 11 years later estimated half a million deaths from COVID-19 in the UK, and whose long-discredited predictions are still being used to justify inflicting an equally unnecessary COVID-19 vaccine on the British people today. Like Oxford University, Imperial College is a beneficiary of the Bill and Melinda Gates Foundation, which has bankrolled it for over a decade, receiving $88.86 million in grants this year alone.
Pandemrix, however, wasn’t just unnecessary. It subsequently emerged that the vaccine can cause narcolepsy and cataplexy in about one in 16,000 people. By 2014, more than 800 children across Europe were known to have been made ill by the vaccine, with more expect to emerge. In the UK, 60 victims were expected to receive around £1 million each in compensation from the Government. 80 per cent of victims were children, but also included NHS staff who had been forced to take the vaccine in order to work. Since GSK had refused to supply the vaccine unless it was first indemnified against claims for damage, it paid the bill then claimed it back from the relevant governments. A decade later, pharmaceutical companies developing the COVID-19 vaccine have demanded the same indemnity.
But that wasn’t the end of GlaxoSmithKline’s long history of malpractice and fines. In 2012, GSK was fined $3 billion — until then the largest settlement in history — after admitting bribing US doctors and encouraging the prescription of unsuitable anti-depressants to children. And in 2016, GSK was fined over £37 million by the Competition and Markets Authority for paying bribes to keep generic varieties of the antidepressant, Paroxetine, out of the UK market. That seems a lot, but that same year GSK made $528 million from Bexsero; and in its EvaluatePharma World Preview 2017, Outlook to 2022, the life-science commercial intelligence firm, Evaluate, projected that sales of Bexsero to 2022 will more than double to $1.17 billion.
A senior figure at GlaxoSmithKline throughout this period was Dr. Patrick Vallance, who joined the company in 2006 as head of drug recovery, rose to head of medicines discovery and development in 2010, and finally, in 2012, was appointed President of Research and Development. In 2018 he left to become Chief Scientific Advisor to the UK Government, was knighted the following year, and in 2020 was appointed Chair of the Scientific Advisory Group for Emergencies. It has subsequently emerged that Sir Patrick left GSK with shares worth £6.1 million at their current value, and still had £600,000 worth of shares in the company, which has deals to supply 60 million doses of a COVID-19 vaccine to the UK Government and 100 million doses with the US Government.
But to return to Professor Andrew Pollard, in April of this year Oxford University entered into a partnership not with GlaxoSmithKline but with the British pharmaceutical company, AstraZeneca, to sell what subsequent deals have established will be 400 million doses of its COVID-19 vaccine in Europe, 700 million to the US and GAVI, and 1 billion doses to India. Their latest figures are for a production capacity of 3 billion doses in 2021. As a result of these deals, AstraZeneca’s net profit in the second financial quarter of 2020 rose to £581.18 million, compared to just £99.94 million in the same quarter last year. This made AstraZeneca the most valuable UK company by market capitalisation, and this October it was still the second most valuable. The COVID-19 vaccine should put them back in first place.
In September of this year, AstraZeneca and Oxford University’s coronavirus vaccine trial was paused after a UK participant suffered spinal cord inflammation; yet it took a month for them to send the vaccine trial safety data to the US Food and Drug Administration (FDA). This was not the first time AstraZeneca has fallen foul of the FDA. Ten years earlier, in 2010, AstraZeneca had paid $520 million in fines to settle charges by the US Federal Government for illegally marketing the anti-psychotic drug Seroquel to children and elderly patients for uses not approved by the FDA. In 2015, it was revealed that pharmaceutical companies were paying UK doctors £40 million every year to promote drugs, with the UK office of AstraZeneca paying £671,400 in fees to 903 doctors plus £30,200 for their travel and hotel bills. Just two years ago, in April 2018, it was revealed that AstraZeneca had paid €17.9 million in secret payments to ‘independent’ healthcare professionals to endorse their products, including the use of vaccines. Indeed, it has just been revealed that AstraZeneca’s claim that its vaccine has an efficacy of 90 per cent is based on a test only administered to individuals aged 55 and below, a demographic with a far lower chance of developing COVID-19 symptoms requiring a vaccine. Since the announcement, London-listed shares in AstraZeneca have lost more than 6 per cent in value. This is the company that will be producing 3 billion doses of the Oxford vaccine for COVID-19. On 8 December, an interim analysis of trials of the ‘safety and efficacy’ of the AstraZeneca vaccine was published in The Lancet, and among the funders was, once again, the Bill & Melinda Gates Foundation, and AstraZeneca itself.
After authorising the use of Bexsero, Professor Pollard has kept his position as Chair of the Joint Committee on Vaccination and Immunisation that advises UK health departments on vaccines; but because of this conflict of interests he recused himself from the first JCVI meeting on COVID-19, and will not take part in Committee discussions about the SARS-CoV-2 vaccine he is developing at Oxford.
3. Professor Jonathan Van Tam
Professor Jonathan Van Tam, who Chairs the SAGE SPI-Modelling subgroup responsible for the lockdowns and other restrictions, is also the UK’s Deputy Chief Medical Officer, a position he assumed in October 2017. Before that, Van Tam was in the pharmaceutical industry, joining the British multinational pharmaceutical company SmithKline Beecham as an Associate Director in 2000; moving to the Swiss healthcare company Roche as Head of Medical Affairs in April 2001; and finally, in February 2002, taking up the position of UK Medical to Aventis Pasteur MSD, the vaccines division of the French multinational pharmaceutical company Sanofi. In 2004 Van Tam returned to the public sector, joining the newly-created Health Protection Agency Centre for Infections, where he was Head of the Pandemic Influenza Office until October 2007.
According to Tom Jefferson in an article published in the British Medical Journalin December 2017 about the revolving doors between public and private positions in healthcare, Professor Van Tam is a regular attendee at conferences organised by the European Scientific Working Group on Influenza (ESWI), a well-known, industry-funded lobbying group. Indeed, his predecessor as Deputy Chief Medical Officer, Professor John Watson, was a founding member of the ESWI. And as head of the Pandemic Influenza Office, Professor Van Tam bears responsibility for decisions that were heavily criticised in 2013 by the Public Accounts Committee regarding the overlapping roles of pharmaceutical companies, lobbyists and regulators in the production, trial and use of the influenza antiviral drug Oseltamivir (Tamiflu). This was one of the highest revenue earners for its manufacturer and Van Tam’s former employer, Roche. From 2006, the UK Government spent millions stockpiling Tamiflu in response to estimates that bird flu would kill 200 million people worldwide, and up to 710,000 people in the UK. In reality, around 600 people have died worldwide, and not a single person in the UK even contracted bird flu. Once again, the modeller who made these highly lucrative predictions was Professor Neil Ferguson.
If you’re wondering why Professor Van Tam is so keen on us taking a COVID-19 vaccine — he has recently resorted to saying he would give it to his 78-year-old mother and be the first in the queue to take it himself were it ethical to do so — £424 million of taxpayers’ money was spent on Tamiflu. Yet of the 123 clinical trials of the antiviral that were conducted, 74 were entirely funded by Roche, its manufacturer; and of those, the European Medicines Agency received just 15 incomplete accounts of trials, and the National Institute for Health and Care Excellence just 4 incomplete accounts of trials. According to an article published in the British Medical Journal, it took Roche 4 years to hand over the full Clinical Study Reports. When they were finally available for scrutiny, these showed that the World Health Organisation (WHO), the European Medicines Agency (EMA) and the US Centers for Disease Control and Prevention (CDCP) had all approved, recommended and encouraged the stockpiling and use of Tamiflu without having first vetted the underlying data. This stockpiling earned Roche billions. Worse still, when this data was reviewed by the Cochrane Review Group, it concluded that there was no convincing trial evidence that Tamiflu affected either influenza complications in treatment or influenza infections in prophylaxis, and raised new questions about the drug’s harms profile.
In the Public Accounts Committee report on ‘Access to clinical trial information and the stockpiling of Tamiflu’ published in 2013, Dr. Fiona Godlee, Editor in Chief of the British Medical Journal, when asked why the UK Government had spent £424 million on a useless vaccine for a viral threat that had never existed, responded:
‘I will give you my brief answer. I think it was politically expedient. There was an outbreak of potentially serious influenza. There was a World Health Organisation recommendation that countries should do this. I should say that there is a whole host of information about what led to that WHO recommendation, with industry-funded advisers helping WHO reach that decision. The UK was confronted with a situation in which it wanted something. There isn’t anything else for pandemic flu. To cut a long answer short, I would say it was bread and circuses to keep the populace happy, and I think it was misleading and wrong, especially as the alternative, paracetamol, is well understood, and Tamiflu has adverse effects, apart from its cost.’
Fast forward 7 years, and we’re back in the same but worse situation. Far from being ‘unprecedented’, as we are constantly being told, health ‘crises’ have been repeatedly manufactured by Big Pharma, with Professor Ferguson its go-to-man for prophecies of doom that have been consistently shown to be wrong by many orders of magnitude. This time, however, we’re entering a new level of corruption and collaboration between the public and private sectors. Compulsory vaccination has always been the goose that will lay a trillion golden eggs for the pharmaceutical industry and its global investors; and on 13 November, Conservative MP Lt. Col. Tom Tugendhat, who Chairs the Committee for Foreign Affairs, called for a COVID-19 vaccine to be made a condition of access to public transport, social venues and places of work. Throughout this manufactured health ‘crisis’, this has been how the Government has leaked future policy to the media to test the public’s reaction. In this case, it looks very much like the first step in the mandating of mass vaccination as part of the programmes and technologies of the UK biosecurity state.
4. Making the World Safe for Vaccines
Finally, as further evidence of how ready the Government is to change legislation to accommodate these programmes, in a consultation document published on 28 August and closed on 18 September, the Department of Health and Social Care canvassed the responses of unidentified ‘stakeholders’ to proposed draft changes to the Human Medicine Regulations 2012, in order to support the issuing, advertising, distributing, selling and administering of COVID-19 vaccines. These changes would:
- Change Regulation 74 to allow the Joint Committee on Vaccination and Immunisation (JCVI) to advise the Government to use a tested but unlicensed vaccine, which will instead be given a temporary authorisation by the UK’s licensing authority, the MHRA.
- Extend the scope of immunity from civil liability already conferred by Regulation 345 — which already indemnifies key actors in the medicines supply chain from being sued in the civil courts for the consequences resulting from the use of an unlicensed product that a national licensing authority has recommended in order to deal with certain specific health threats (which it calls ‘unfair’) — to provide ‘complete immunity’ not only to manufacturers and healthcare professionals but also to the pharmaceutical companies placing an unlicensed medicine such as a COVID-19 vaccine on the market.
- Extend the workforce permitted under Regulation 214 to administer both the unlicensed COVID-19 vaccine and the expanded influenza vaccine from just doctors and other registered healthcare professionals to include midwives, nursing associates, operating department practitioners, paramedics, physiotherapists and pharmacists.
- Disapply Part 14 of the Human Medicines Regulations to allow unlicensed medicine or medicinal product, such as the COVID-19 vaccine, to be promoted and advertised to both healthcare professionals and the public by the suppliers, and to permit such suppliers to participate in any public information campaign relating to the use of the medicine.
- To remove the requirement, under Regulation 18, for distributors of an unlicensed medicine, including the COVID-19 vaccine, to have a wholesale dealer’s licence. Such exemptions would be provided for service providers contracted by the NHS and the Armed Forces.
These proposed changes, which the DHSC justifies on the grounds of what it calls ‘the biggest threat this country has faced in peacetime history’, are not, however, limited to a COVID-19 vaccine, but ‘will also facilitate the efficient mass distribution of treatments for . . . any other disease that poses a serious risk to public health.’ On 16 October, these proposals were made into law by the Human Medicines (Coronavirus and Influenza) (Amendment) Regulations 2020. On 31 December the Vaccine Damage Payments (Specified Disease) Order 2020 added COVID-19 to the list of diseases against which payments made to individuals who are severely disabled as a result of vaccination are limited to a one-off, tax-free, Vaccine Damage Payment of £120,000. Following their £3,360 pay rise to an annual salary of £85,291, that’s the equivalent of an MP’s salary for less than 17 months, not including their income as lobbyists, consultants and board members of pharmaceutical companies and healthcare firms. Since the vaccine manufacturers, non-registered health professionals administering it and pharmaceutical companies selling it are all indemnified from such claims, this sum would be paid by the UK Government.
On 20 November, a study published in Nature Communications, one of the world’s most highly regarded peer-reviewed journals, titled ‘Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China’ reported that, out of 9,899,828 residents and 92.9 per cent of the population of Wuhan tested between 14 May and 1 June a month after lockdown restrictions were lifted on 9 April, no new symptomatic cases and just 300 asymptomatic cases were identified. From the latter, no positive tests for SARS-CoV-2 were identified among 1,174 close contacts of asymptomatic cases. Further testing of 52,312 samples between 13 June 13 and 2 July found no positive results; and two months after the screening of nearly 10 million residents, by 9 August there were still no newly confirmed cases of COVID-19 in the city most severely affected by COVID-19 in China. Statistically speaking, although there are some documented instances, the asymptomatic transmission of SARS-CoV-2 doesn’t exist as a vector of infection requiring a vaccine.
What we’re threatened by in the UK is not a virus but an epidemic of tests which, as I’ve covered in detail in my previous article, The Betrayal of the Clerks, have a far higher False Positive Rate (median of 2.3 per cent) than the 1.22 per cent of the population currently identified by those tests as having SARS-CoV-2. This includes those who have died of some other medical cause. As of 18 November, the NHS reports just 1,664 people whose deaths have been attributed to COVID-19 dying in English hospitals this year without a pre-existing medical condition. The so-called ‘second wave’ of ‘COVID-19 deaths’ is consistent with the annual rise in overall mortality in the UK at this time of year, particularly from respiratory diseases, which have inexplicably dropped over the four weeks to 13 November, the same weeks in which deaths attributed to COVID-19 have risen. In the same 4 weeks last year there were 5,399 deaths from respiratory diseases; this year there are 3,958.
Equally, the current slight increase in overall mortality over the five year average must be placed in the context of the effects of the ongoing reduction and withdrawal of medical care and treatment for the elderly and sick throughout this year. Back in July, after the 16,000 excess deaths in March and April not attributed to COVID-19, a report published by the Department of Health and Social Care, the Office for National Statistics, the Government Actuary’s Department and the Home Office estimated a further 26,000 excess deaths this year resulting from coronavirus-justified changes to emergency and adult social care, with thousands of additional deaths resulting from the postponement of diagnoses and cancellation of treatment and operations.
To take just one of the major causes of death in the UK increased by Government imposed changes to healthcare, the British Medical Journal reported this month that even a month’s delay in cancer surgery increases the risk of death by 6-13 per cent, with a 3-month delay increasing the risk by approximately 25 per cent, rising to 44 per cent for treatments like bowel cancer chemotherapy. As winter draws in, and the deaths not only from cancer but also from heart disease (25.9 per cent increase in deaths), diabetes (47 per cent increase in deaths) and dementia (79 per cent increase in deaths) mount up, only to be attributed to ‘COVID-19’ by a testing programme unfit for any purpose other than to mislead the public, the Government’s criminal decision to restrict and withdraw medical care for life-threatening conditions is beginning to reap its bloody harvest.
Against this indefensible massacre of the innocents in the circus of political expediency, the need for a vaccine for COVID-19 into which the Government has already sunk over £6 billion of public money would appear to exist only in the minds and wallets of the doctors, scientists, universities, government departments, executive agencies, regulatory bodies, pharmaceutical companies and global investors who will benefit and profit from producing, guaranteeing, advertising and enforcing a vaccine for COVID-19 — and any other threat to public health they can conjure into being — on the population not only of the UK but of the world.
Even to suggest this, however, or to ask the numerous questions the documented and verifiable evidence in this article must raise in the minds of the British public, means I and anyone sharing this article online can be censored or shut down by Government Communications Headquarters (GCHQ). This month the intelligence and security organisation launched a cyber offensive targeting social media accounts publishing content deemed ‘propaganda’ merely for raising concerns about COVID-19 vaccine development and the pharmaceutical companies and global investors involved. And if GCHQ reportedly being told by the UK Government to ‘take out’ anyone who questions the medical necessity or financial motivations for a COVID-19 vaccine (something it denounces as ‘vaccine hesitancy’, as if anything besides blind and immediate obedience is now a crime) wasn’t enough of a deterrent, the Labour Party has now called for emergency legislation to issue criminal and financial sanctions against social media platforms that don’t censor anyone who does so.
But if the UK biosecurity state has to threaten people with being ‘extremists’ and a ‘national security risk’ in order to make us take the COVID-19 vaccine, we are within our rights — and in possession of our senses — to ask what cheerleaders like Dr. June Raine, Professor Andrew Pollard and Professor Jonathan Van Tam are hiding behind their brightly-coloured pompoms.
Addendum: How Safe is the AstraZeneca Vaccine?
Under recent changes to the Human Medicines Regulations 2012, the Oxford/AstraZeneca vaccine for COVID-19 has been granted ‘temporary authorisation’ for use in the UK; but its long-term effects are still unknown, so it is unapproved and experimental. But what does this mean?
The European Medicines Agency (EMA) has published ‘Human medicine European public assessment report (EPAR): COVID-19 Vaccine AstraZeneca’. This was last updated on 18 February, and so represents a summary of the latest data on this product at the time of publication. 4 clinical trials of 24,000 people across the UK, Brazil and South Africa showed a 59.5 per cent reduction in the number of symptomatic COVID-19 cases in people given two doses of the vaccine, with the second dose given 4-12 weeks after the first. This equates to around 60 per cent ‘efficacy’. However, most of the participants in these studies were 18-55 years old. There were not enough results in participants over 55 to provide a figure for how well the vaccine will work in this age-group. More information is expected from ongoing studies with elderly participants.
Although there were no additional side effects in the 345 people who received COVID-19 Vaccine AstraZeneca in the trials and had previously had COVID-19, there was not enough data from the trials to conclude how well the AstraZeneca vaccine works on people who have had COVID-19.
The impact of vaccination with the AstraZeneca vaccine on the spread of SARS-CoV-2 is not yet known, and will only emerge from the UK programme of mass vaccination. It is also not yet known to what extent vaccinated individuals may still be able to carry and spread the virus.
It is also not known how long protection given by the AstraZeneca vaccine lasts. Those vaccinated in the clinical trials will continue to be followed for one year to gather more information on protection.
The AstraZeneca vaccine is currently not recommended for use on children; but the EMA has agreed with the pharmaceutical company on a plan to conduct trials on children at a later stage. There is still limited data on the vaccine’s effects on people with weakened immune systems.
Information on the use of the AstraZeneca vaccine on patients with co-morbidities (such as chronic obstructive pulmonary disease, diabetes, chronic neurological disease, cardiovascular disorders), or on those with autoimmune or inflammatory disorders, is currently classed as ‘missing’.
Preliminary studies on animals do not show any harmful effects on pregnancy. However, data on the use of the AstraZeneca vaccine during pregnancy is still very limited.
Allergic reactions (hypersensitivity) have been observed in people receiving the AstraZeneca vaccine; and it is currently recommended that participants who have a severe allergic reaction when they are given the first dose should not receive the second dose.
The safety, immunogenicity, and efficacy of the AstraZeneca vaccine when co-administered with other vaccines has also not been evaluated. Because of the rushed nature of the clinical development program, understanding of the long-term safety of the product is currently described as ‘limited’.
Despite this uncertainty, on 29 January, the AstraZeneca vaccine was granted a ‘Conditional marketing authorisation’ by the European Medicines Agency. This is the approval of a medicine that addresses unmet medical needs of patients on the basis of less comprehensive data than is normally required. To be granted such authorisation, the available data must indicate that the medicine’s benefits outweigh its risks, but implies that there is more evidence to come about the vaccine, which the pharmaceutical company is required to provide from the clinical trials, which are ongoing.
Until this evidence is produced, the European Medicine Agency has produced a ‘European Union Risk Management Plan’ for the AstraZeneca vaccine (drug substance: ChAdOx1-S (recombinant), AZD1222), which contains information about the vaccine’s safety. This plan includes a list of Adverse Events of Special Interest for the AstraZeneca vaccine. These are adverse reactions that may be of interest in the context of a mass COVID-19 vaccine administration campaign for COVID-19, such as the one currently being carried out in the UK. The list of Adverse Events of Special Interest (AESIs) applicable to the AstraZeneca vaccine that had been established from research and clinical trials by 4 November, 2020, 3 months before it was authorised for temporary use, include the following.

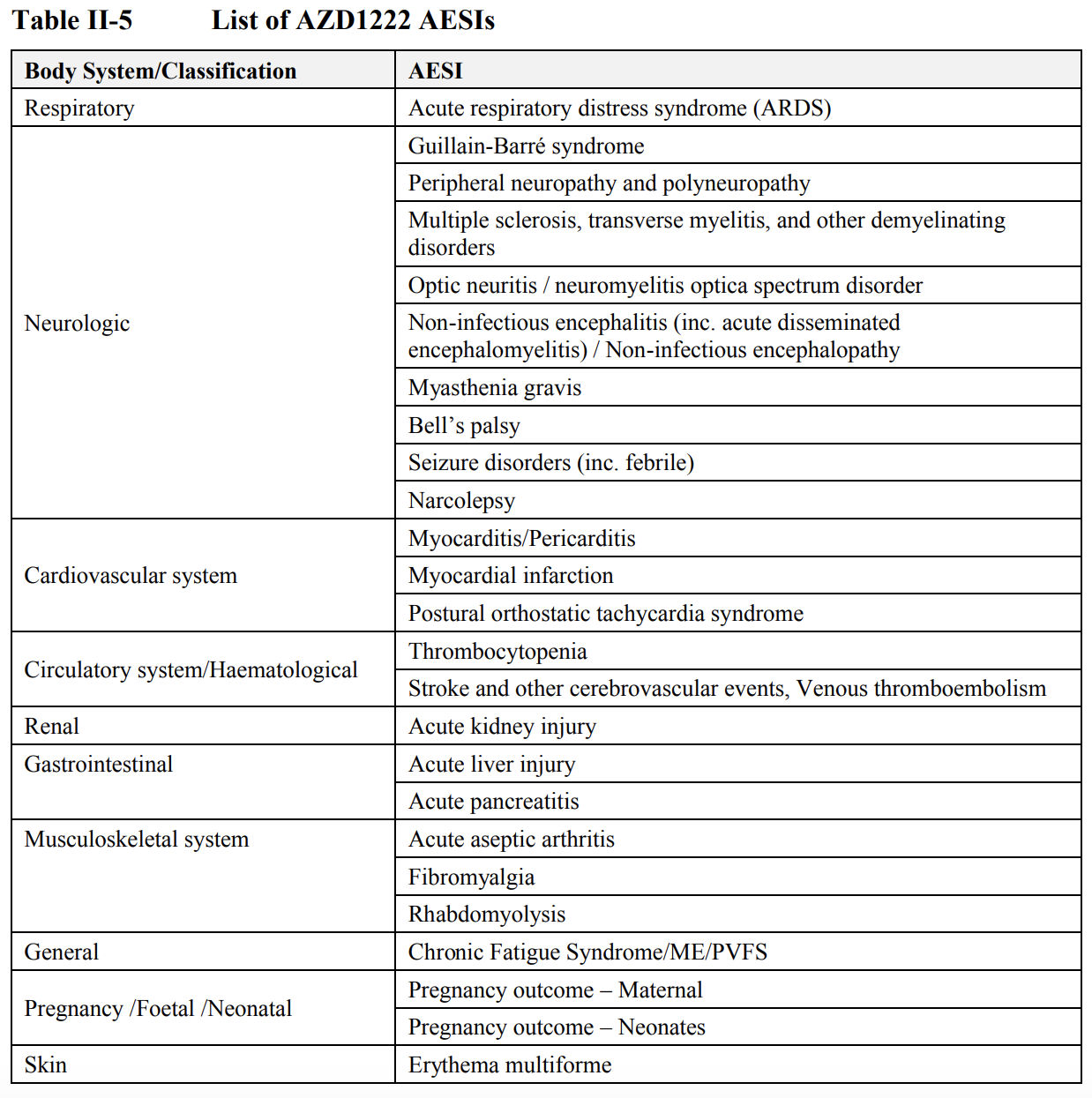
As of 21 February, 2021, 8.4 million first doses of the AstraZeneca vaccine have been administered in the UK. The Medicines and Healthcare products Regulatory Agency has received 42,917 reports of 157,637 suspected adverse reactions (ADRs). 244 of these were of the participant dying shortly after vaccination. Of these ADRs, 1,516 were cardiac disorders (of which 30 were fatal); 17,597 gastrointestinal disorders (5 fatal); 3,016 infectious disorders (32 fatal); 2,057 metabolic disorders (2 fatal); 34,656 disorders of the nervous system (14 fatal); 4,059 respiratory disorders (10 fatal), and 56,377 general disorders (146 fatal). In total, including the BioNTech/Pfizer vaccine, out of 18.4 million doses administered in the UK, there have been 242,651 ADRs resulting in 460 deaths occurring shortly after vaccination.
Simon Elmer
Architects for Social Housing
Further reading by the same author:
Cui Bono? The COVID-19 ‘Conspiracy’
Lies, Damned Lies and Statistics: Manufacturing the Crisis
Our Default State: Compulsory Vaccination for COVID-19 and Human Rights Law
Bowling for Pfizer: Who’s Behind the BioNTech Vaccine?
The Betrayal of the Clerks: UK Intellectuals in the Service of the Biosecurity State
When the House Burns: Giorgio Agamben on the Coronavirus Crisis
The Infection of Science by Politics: A Nobel Laureate and Biophysicist on the Coronavirus Crisis
The New Normal: What is the UK Biosecurity State? (Part 2. Normalising Fear)
The New Normal: What is the UK Biosecurity State? (Part 1. Programmes and Regulations)
The Science and Law of Refusing to Wear Masks: Texts and Arguments in Support of Civil Disobedience
Lockdown: Collateral Damage in the War on COVID-19
Manufacturing Consensus: The Registering of COVID-19 Deaths in the UK
Giorgio Agamben and the Bio-Politics of COVID-19
Good Morning, Coronazombies! Diary of a Bio-political Crisis Event
Coronazombies! Infection and Denial in the United Kingdom
Language is a Virus: SARs-CoV-2 and the Science of Political Control
Sociology of a Disease: Age, Class and Mortality in the Coronavirus Pandemic
![]()

Exceptional article, thank you, packed with important information, especially (but not only) with regard to conflicts of interest. Recommend printing it out.
LikeLike
Really great article! Thank you for sharing and providing so many references.
LikeLike
The Nature Comms article you cite on Wuhan (not Nature as you say, although still a “prestigious” journal) – this relies on 9,899,828 PCR tests carried out in less than a month, via the same assay that everyone else is using. Based on the other things I’ve read here on PCR testing: where have all the false positives gone?
LikeLike
Although Dr. Mike Yeadon (see our article on The Betrayal of the Clerks) has pointed out that not everyone infected with SARS-CoV-2 will produce antibodies, especially when the viral dose has been weak, the Nature Communications article reports that 190 of the 300 asymptomatic ‘cases’ had a positive Immunoglobulin G, the most common antibody, which protects against bacterial and viral infections. This indicates that 63.3% of the asymptomatic positive cases were actually infected. However, 36.7% of the asymptomatic ‘cases’ had negative Immunoglobulin G and M, ‘indicating the possibility of infection window or false positive results of the nucleic acid testing’.
In considering the limitations of the study, the authors conclude that ‘although a positive result of nucleic acid testing reveals the existence of the viral RNAs, some false negative results were likely to have occurred, in particular due to the relatively low level of virus loads in asymptomatic infected individuals, inadequate collection of samples, and limited accuracy of the testing technology.’ However, they point out that ‘even if test sensitivity was as low as 50%’ (a meta-analysis reported a pooled sensitivity of 73%), ‘then the actual prevalence would be twice as high as reported in this study, but would still be very low.’
Importantly, for the RT-PCR tests used in Wuhan, a cycle threshold value (Ct-value) less than 37 was defined as a positive result, and no Ct-value or a Ct-value of 40 or more was defined as a negative result. For Ct-values ranging from 37 to 40, the sample was retested. If the retest result remained less than 40 and the amplification curve had obvious peak, the sample was classified as positive; otherwise, it was reported as being negative. These diagnostic criteria were based on the Chinese Government’s official recommendations.
In comparison, in the UK the False Positive Rate has not been disclosed by the Government; but Public Health England’s guide for health-protection teams published in October, ‘Understanding cycle threshold (Ct) in SARS-CoV-2 RT-PCR’, it states that ‘a typical RT-PCR assay will have a maximum of 40 thermal cycles.’ In the Wuhan test scheme, these would all qualify as a negative result.
I think the difference is that, in China, the Government is trying to establish the minimum safety requirement required to get the population back to work; whereas in the UK the Government is trying to keep the population out of work for as long as possible, and only to allow us back to work on the condition of our compliance with the programmes and technologies of the biosecurity state, including mandatory vaccination, immunity passports, mask wearing, contact tracing, health monitoring, etc.
So although there are ‘indications’ of false positives in the Wuhan tests, it wasn’t what the authorities were looking for; whereas in the UK our entire Test and Trace programme, and the erasure of our civil liberties it justifies, is based on the production of thousands of False Positives. In the PHE guide it states very clearly that ‘RT-PCR detects presence of viral genetic material in a sample but is not able to distinguish whether infectious virus is present’ (p. 6). The RT-PCR test was never designed either to prove infection or to diagnose an infectious disease. What it is very good at, however, is what it is being used by the UK Government to do, which is produce 100% false positives for a virus that has all but disappeared from the country.
Click to access Understanding_Cycle_Threshold__Ct__in_SARS-CoV-2_RT-PCR_.pdf
LikeLike
I cannot praise this article enough.
The layout, the sourcing, the presentation and the logic are impeccable and are just what is needed at the present moment to awaken the victims of this political manipulation and consequential economic ruin to the situation they are in.
Except that they cannot be awakened! And will not be before it is too late.
Please don’t be disheartened, though. There are many (if proportionately few) who will see and be able to take precautions to prepare themselves and hopefully join in the efforts of those like you who are sounding your warnings.
Please don’t think I am being facetious when I say that, on an almost equally vast and serious historical landscape, it has echoes of Karl Marx and Das Kapital. Then, the few who had the education to see what was happening in terms of the exploitation of the disadvantaged by the greed and unscrupulousness of the powers that be, were unable to reach the awareness levels of the victims until violence entered the equation on a level which subsequently produced revolution and war.
It could happen again. Please keep up your good work.
Brian Taylor
LikeLike
The share price of GSK, AZ and Pfizer are down or flat compared to January. They aren’t in it for the money
LikeLike
GlaxoSmithKline started the year at £17.77 a share and has fallen to £13.74. AstraZeneca started at £76.66 and is now on £79.58, having fallen from £87.85 on 11 November when it looked like it would be the first pharmaceutical company to release a vaccine for COVID-19, before it was revealed they’d lied about the tests. Pfizer started the year at $37.08 and is now on $40.34, having risen from $35.36 on 16 November, shortly before they announced the COVID-19 vaccine.
So what you’ve said is factually incorrect. The share price of these pharmaceutical companies this year is directly linked to their success in finding an unlicensed vaccine for COVID-19 and how it’s been greeted by the market. I don’t know whether your incorrect assertion is because you haven’t bothered to look at the statistics or because you’re trying to dismiss with unfounded assertions the valid questions I’ve raised in this article about the rapidity of the vaccine’s production, the inadequacy of its testing, the financial motivations and history of corruption of all the individuals, companies and government organisations involved in this race for a COVID-19 vaccine, let alone the need for it or how legislation is being changed by the UK Government to accommodate and, possibly, mandate it. But either way, your assertion that some of the most powerful and wealthy companies in the world, which have repeatedly broken the law and paid millions and – in the case of GlaxoSmithKline and Pfizer – billions in out-of-court settlements to escape prosecution for malpractice and manslaughter, ‘aren’t in it for the money’ shows your naivety about the pharmaceutical industry and the revolving door between it and Government regulators.
Unfortunately, however, the manufacture of this coronavirus isn’t merely about the vast sums these companies are going to make selling needless and unlicensed vaccines for a virus that presents a threat to a tiny proportion of the population and has the fatality rate of seasonal influenza, but is also about the political control being exerted through the requirement to take such vaccines on the basis of the naivety and ignorance you’ve demonstrated.
I have left your comment here to demonstrate how easy it is to refute these bullish assertions of falsehood, but if you wish to make any further comments please do some research and thinking first. Thank you.
LikeLike
Seroquel is now routinely given – in some cases forced – for anxiety and sleep by psychiatrists in the UK, although it is not licensed for anxiety. It is a dangerous drug and disgustingly life draining to experience. Discribed as torture (akathisia) by those on it. So you can expect people who have suffered stress anxiety insomnia over all these lockdowns to be on the wrong end of this drug.
LikeLike
The total corruption is legendary. Most of the people mentioned in this article should be ashamed of themselves, but as they are the vermin of the earth, parasites and posers, they cannot have a soul to care.
LikeLike
Very good piece with detail …. appreciated. Hopefully many of these reprobates will find themselves in front of a military court and get their just deserts. Unfortunately corruption is total and Government deep and they will all keep getting away with it especially when the Globalist Coups finally manifest themselves. From what has been happening in this sector a Coup would be relatively easy to pull off from the information you have laid out.
LikeLike