This is the third in the series of articles I’m writing about what has become known as the coronavirus pandemic. In the first, COVID-19 and Capitalism, I argued that the UK Government’s decision to send workers home without pay while compensating businesses for lost revenue with vast sums of public money was capitalism attempting to recoup its losses to the suspension of commerce and the resulting fall in share prices caused by the spread of the pandemic. For someone who researches and writes about housing policy that claims to address the crisis of housing affordability in the UK while reproducing and expanding it this was familiar territory for me. In my second article, however, Sociology of a Disease, I had to be more circumspect. Epidemiology is definitely not my field, and I started by analysing the figures being published every day about the number of cases of infection in each country, the number of new cases, the total deaths, the new deaths, the number of people recovered, and the various other figures extrapolated from these, such as the number of cases per million of the population. By the time I’d finished I was beginning to doubt my own conclusions — which one always should — that went against everything being said by our Government and published in our media. That in itself was hardly surprising when the latter has become completely subsumed into a propaganda arm of the former in the UK; but in the week after publication my continuing research led me to the growing body of scientific opinion across the world that contradicts the official narrative on the coronavirus; and by the end of the week it was incontrovertible: the extent and threat of the pandemic is being enormously and deliberately exaggerated by governments, their scientific advisors and the press and media. Under a title coined by William S. Burroughs and made famous by Laurie Anderson, this article looks at how this is being done, what consequences it has already had for our loss of civil liberties, and what further consequences it might have in the future. It’s grim reading, and tells an alarming story of our susceptibility — not only as a nation but as a global and historical configuration — to the full spectrum of technology by which we are controlled by the workings of power. But if you’re sick of being a guinea pig for this epidemic of mass panic, this may be the antidote you need.
1. Infection Rate
Among the myriad statistics being published every day to induce the mass panic we’re seeing, one anomaly has been little commented upon. One of the highest rates of positive tests for coronavirus in the world, at 3,865 cases per million of the population, is not Italy, with 1,906, not Spain, with 2,397, and definitely not the UK, with 497, but Iceland. With a population of only 340,680 that’s only 1,319 cases compared to over 115 thousand in Italy, 112 thousand in Spain, and nearly 34 thousand in the UK; but proportionately, according to these figures published on various websites recording the daily spread of the pandemic, Iceland is the worst infected.
What, Iceland!, you say. If there is any country in Europe, which contains 7 of the 10 worst infected countries, likely to be least affected by the pandemic it is Iceland. Isolated in the North Atlantic Ocean 1,400 miles from mainland Europe, Iceland only reported its first case of the virus on 27 February, by which time Italy had over 650 cases, and even the UK had 16. So how did this epidemic sweep so virulently across the land of ice and snow?
The answer, of course, is very simple. With the 6th smallest population in Europe, a universal health care system with no private hospitals and little private insurance, the 11th highest expenditure on health care as a percentage of GDP in the world, and a government policy of testing as many of its citizens as possible for novel coronavirus, Iceland has produced what is so far the most accurate data available about the pandemic.
As of 1 April, 20,930 samples have been taken by the National University Hospital of Iceland, representing 1 in every 16 people. Of these, 1,319 have tested positive for novel coronavirus, or around 1 in 16 samples. According to Thorolfur Guðnason, Iceland’s Chief Epidemiologist at the Directorate of Health, about half of those who tested positive show no-symptoms, and the other half displays ‘very moderate, cold-like symptoms.’ A tiny minority, 44 out of nearly 1,100, are currently in hospital, 12 of whom are in intensive care. So far, only 4 people in Iceland have died after testing positive for coronavirus: one a tourist who died of unknown causes atypical of COVID-19, another of a long-term illness.
So, what do these figures tell us about the infection rate of Severe Acute Respiratory Syndrome Coronavirus 2 (SARs-CoV-2), which causes — but is not the same thing as — Coronavirus disease 2019 (COVID-19), and about the mortality rate of the latter?
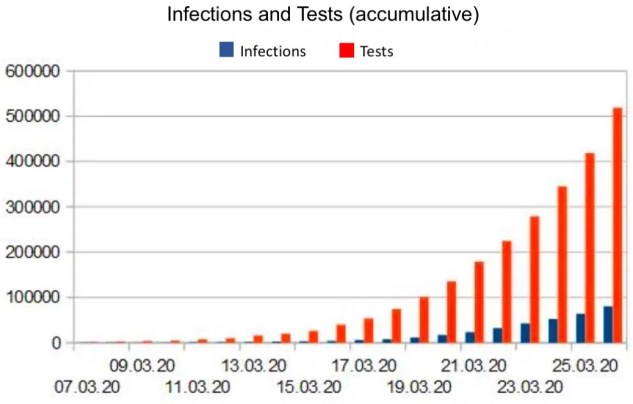
First, they tell us that case numbers are a product of testing. One of the principles of quantum mechanics is that the observer determines the observed, and the more we test for the presence of novel coronavirus the more we find it present. Presumably, if Iceland continues to keep testing all its citizens, eventually it will be shown that 1 in 16 or a higher share of the population has contracted the coronavirus. However, that will not increase the numbers who die with SARs-CoV-2 in their body, and still less those who die as a result of COVID-19. On the contrary, as the German researcher, Dr. Richard Capek, has shown in an ongoing series of comparative analyses of data from the USA, the proportion of samples testing positive for SARs-CoV-2 has been between 5 and 15 per cent, which corresponds to the usual spread of corona viruses. And as the number of tests has increased exponentially, so the number of infections has remained constant and proportional (below), while the rate of mortality has decreased. This data does not suggest the exponential spread of a viral pandemic, but rather what Dr. Capek describes as an ‘epidemic of tests’.
Second, the figures from Iceland tell us that the mortality rate from COVID-19 is as low as or lower than other corona viruses, and lower than that from seasonal influenza, and nothing like the epidemics in Germany in 2017-18, when there were over 25,000 excess deaths attributable to influenza-related illnesses; in Italy in 2016-17, when there were nearly 25,000 excess deaths; or in England in 2014-15, when there were over 28,000 excess deaths. Needless to say, none of these worse-than-average mortality rates from seasonal influenza — which greatly exceed the 1,107, 13,915 and 2,921 deaths attributed to COVID-19 in these countries as of 2 April — occasioned their governments’ current suspension of the populations’ civil liberties.
2. Mortality Rate
But how can this be true, when the papers are full of claims by NHS staff that the official death count in the UK is not reflecting their experiences on the wards of our hospitals, and social media is awash with photographs of masked staff pleading with us to ‘stay home and save lives’?
After the Grenfell Tower fire there was a strange phenomenon. The North Kensington community immediately challenged the official estimate of the number of people who died as a result of the fire, either in the building itself or afterwards as a result of smoke inhalation. Because of the number of immigrants living unregistered in Grenfell Tower, and because of the number of Muslims visiting friends and relatives during Ramadan on the night of the fire, wild speculations that hundreds had died found wide acceptance and even insistence. Even after investigators had interviewed every survivor about who was with them on the night of the fire and forensic scientists had completed the gruesome task of identifying the charred remains to establish a final death toll of 72, this number continues to be challenged, as if this terrible loss — the highest from a residential fire in the UK since World War Two — was not sufficient to express the full extent of the grief.
With this in mind, let’s look at the daily figures for coronavirus deaths in the UK being published by the Department of Health and Social Care and Public Health England. These report that, as of 2 April, 163,194 people have been tested for coronavirus in the UK, of which 33,718 cases have tested positive, and 2,921 have died. That’s an infection rate of 1 in every 4.8 people tested resulting in a mortality rate of 1 in 11.5. It’s these proportions, updated on government websites every day, printed across the front pages of our daily newspapers in bold letters, and circulated in immediately retweeted memes on social media, that has caused the current panic and terrified obedience to government instructions.
But let’s have a closer look at what these figures represent. Since only 1 in 416 of the UK population has been tested for the coronavirus, compared to 1 in 16 in Iceland, the rate of mortality to infection is all but meaningless. Add to this the fact that the vast majority of those being tested in the UK are in hospital, already ill, and usually from pre-existing medical conditions, and these figures become even more so. According to Sunetra Gupta, Professor of Theoretical Epidemiology at the University of Oxford, in a report she led based on modelling by Oxford’s Evolutionary Ecology of Infectious Disease group, the coronavirus may have reached the UK in mid-January — far earlier than when the first figures were officially compiled at the end of February — and that as much as half of the UK population could already be infected with SARs-CoV-2 without showing any symptoms. This study was challenged by a number of scientists from both the UK and Italy on the grounds that its estimates were based on theoretical speculations rather than empirical data; but until everyone in the UK has been tested for the coronavirus, the figures published by the government to suggest a mortality rate of 1 death for every 11.5 people infected with SARs-CoV-2 is just as speculative and far more irresponsible.
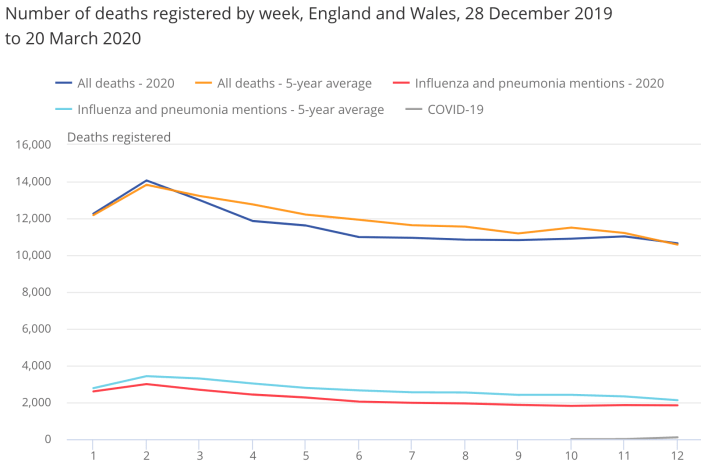
But that’s not all that’s wrong with how the UK government is reporting the extent and threat of the so-called coronavirus pandemic. The Office for National Statistics (ONS), which is semi-independent of the Government, and presumably concerned about this blatant mis-use of statistics to terrify the UK population, announced on 31 March that it will now be providing a separate breakdown of the numbers of deaths involving COVID-19 to its usual, ongoing record of ‘Deaths registered weekly in England and Wales’. Given the extent of the data, there is a time lag between the dates of deaths and their publication, but in the week ending 20 March 2020 — week 12 of the year — there were 10,645 deaths in England and Wales. In comparison, the average number of deaths for the corresponding week over the previous five years, 2015-19, was 10,573 — so the increase on previous years is minimal.
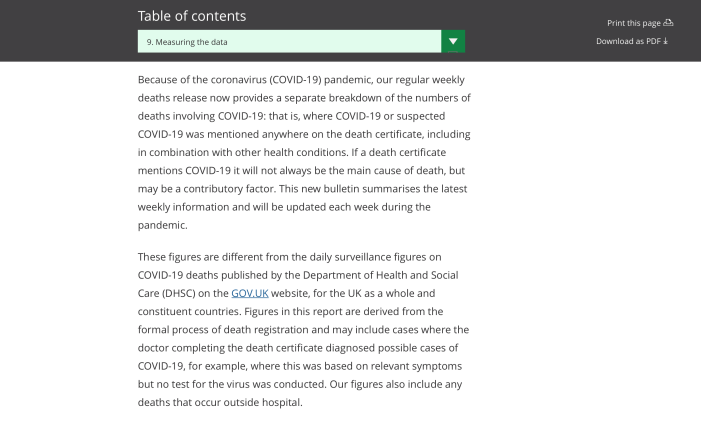
More importantly, in line with its new policy, the ONS reported that, of the deaths registered in week 12, 103 mentioned ‘COVID-19’ or ‘suspected COVID-19’ somewhere on the death certificate. This made up 1.0 per cent of all deaths. However — and this can’t be overemphasised — the Office goes on (below) to clarify that, just because a death certificate ‘mentions’ COVID-19, this doesn’t mean it will always be ‘the main cause of death’. Sometimes it will be a ‘contributing’ factor when ‘combined with other health conditions’. Sometimes the doctor completing the death certificate diagnosed ‘possible cases of COVID-19’ — for example, where this was based on ‘relevant symptoms’ but no test for the virus was conducted. Sometimes the deceased will simply have tested positive for SARs-CoV-2, but a post mortem hasn’t established the actual cause of death.
Yet, extraordinarily, none of the figures recording the ‘number of deaths’ from COVID-19 being published by the Department of Health and Social Care and circulated in the media make any distinction between these possibilities. All the DHSC says of the 2,921 deaths it published on 2 April is that they represent ‘those hospitalised in the UK who tested positive for coronavirus’; while Public Health England, in a pretty well-hidden link ‘About the data’, states that ‘the figures shown are deaths in NHS-commissioned services of patients who have had a positive test result for COVID-19.’
To put the range of inaccuracy inherent in this lack of information in context, the ONS has made a comparison between the number of deaths this year in which COVID-19 has been mentioned as a possible or contributing cause of death or at least been present in the body of the deceased, and the number of deaths from influenza and pneumonia in previous years (below). The reason for making this comparison, they state, is that, unlike coronavirus disease 2019, influenza and pneumonia are both ‘a well-understood cause of death involving respiratory infection that is likely to have similar risk factors to COVID-19.’ And what they have found is that, in week 12 of 2020, while 18 per cent of all death certificates mentioned either COVID-19 (103), or influenza and pneumonia (1,841), or both, in the same week over the past five years an average of 20 per cent of death certificates mentioned influenza and pneumonia (2,120).
3. The Italian Crisis
But this was two weeks ago, you will say, when the virus had barely reached these shores, and since then the death toll has risen to 2,921. Surely this is evidence of a growing epidemic in the UK, and soon deaths from COVID-19 will outstrip those from influenza and pneumonia?
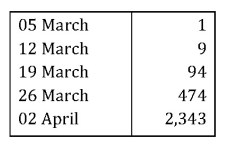
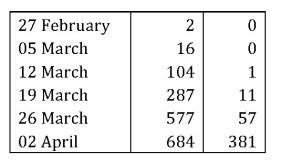
To answer this, let’s go back and remind ourselves how many people have died this year in England and Wales where the underlying cause of death was respiratory disease. These are the figures from the Office for National Statistics for the weeks ending:
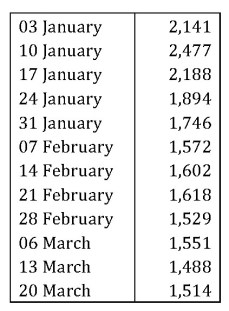
In comparison, these are the number of weekly deaths in the whole of the UK in which COVID-19 is mentioned on the death certificate as a possible or contributing cause, or in which the deceased tested positive for the virus, for the weeks ending:
It will be argued, however, that the first death in the UK attributed to COVID-19 was only registered on 5 March, so we’re only four weeks into a sharply-rising rate of mortality. For a better estimate of the threat of coronavirus, shouldn’t we look to Italy, the worst affected country in the world so far?
There’s a meme that was going around social media but has now been quietly dropped that adopted and promoted this view. According to a comparable table of deaths from coronavirus in Italy and the UK, we were 14 days behind Italy, and in two weeks we would be suffering at the same rate. Apart from the fact that, on 15 February, Italy had 3 cases of infection and the UK 9, making this comparison inaccurate in rate of infection, the rate of deaths has turned out to be very different. Since, on 19 March, Italy had 3,405 deaths from the coronavirus, on 2 April the UK should have had the same, whereas the official number of deaths is 15 per cent lower.
Nonetheless, applying the same criteria, these are the number of weekly deaths in Italy in which COVID-19 was mentioned on the death certificate as a possible or contributing cause, or in which the deceased tested positive for the virus pre- or post-mortem, for the weeks ending:
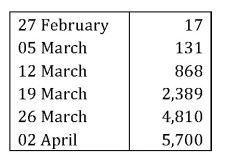
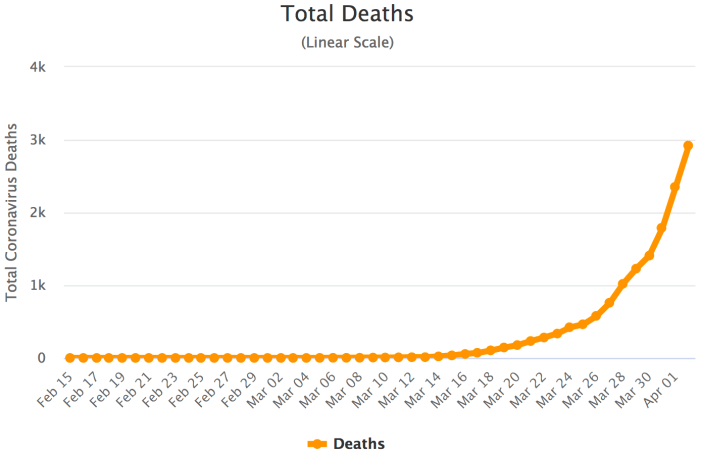
Here, at last, is the evidence of a pandemic, in death rates more than double the worst weeks for deaths from influenza and pneumonia in England and Wales this year. Here is the steepening curve of mortality that awaits us, and which is captured in the charts published on websites like Worldometer (below).
4. Direct Causality from Coronavirus
However, Professor Walter Ricciardi, President of the Italian National Institute of Health — and also one of the signatories to the letter to the Financial Times questioning the lack of empirical data for the estimates in the study by Oxford University — has stated in a widely-repeated comment that:
‘The way in which we code deaths in our country is very generous, in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus. On re-evaluation by the National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus, while 88 per cent of patients who have died have at least one pre-morbidity — many had two or three.’
This, we should recall, is from the scientific adviser to the Minister for Health in the country worst affected by the so-called coronavirus pandemic, which on 1 April, according to the statistics published across the world, has suffered nearly 14,000 of the more than 53,000 deaths from COVID-19. That said, just as it is speculation to map exponential growth in death rates in Italy onto the future of the UK, so it is speculation to apply this 12 per cent causal relation between official deaths and the coronavirus. However, until the Department of Health and Social Care and Public Health England starts publicising the actual causes of death of people who tested positive for SARs-CoV-2, or who displayed symptoms similar to COVID-19, or for which it may have been a possible or contributing cause, this is the best we have to go by as a corrective to the huge range of inaccuracy inherent in these speculations.
As some justification for doing so, we can first compare the data on something not the UK Government but the Office for National Statistics is now providing, and that is the age of all the deceased bundled into this category of ‘death by coronavirus’. This will at least give us a better understanding of who is dying, if not of what they are dying. Up to 20 March, the most recent figures available from the ONS, there were a total of 108 deaths in England and Wales (out of a total of 177 in the UK). Of these, 1 was under 44 years old; 7 were 45-64; 21 were 55-74; 34 were 75-84; and 45 were over 85 years old. This means that 73 per cent of deaths in the UK in which COVID-19 was mentioned as a possible or contributing cause of death, or in which the deceased tested positive for SARs-CoV-2 or displayed similar symptoms to COVID-19, were over 75, and 40 per cent over 85 in a country where the life expectancy is on average 81 years old.
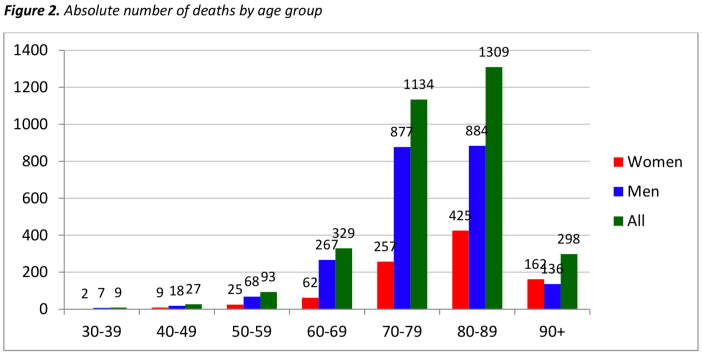
Comparing these figures with Italy, according to the most recent figures available from the Istituto Superiore di Sanitá (above), as of 20 March — using data from 3,199 people who had officially died of coronavirus — 9 were between 30-39; 27 were 40-49; 93 were 50-59; 329 were 60-69; 1,134 were 70-79; 1,309 were 80-89; and 298 were over 90. This means that 85.6 per cent of fatalities, 2,741 deceased, were over 70, with a median age at death of 80 in a country where the life expectancy is 83. Given this close correspondence between the age of the deceased who died testing positive for SARs-CoV-2, there is some justification, therefore, for mapping the 12 per cent causality rate from these deaths in Italy onto those in the UK. Doing so gives us the following estimated deaths from COVID-19, rather than testing positive for SARs-CoV-2, in Italy (left-hand column) and the UK (right-hand column) for the weeks ending:
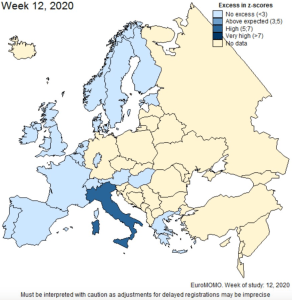
That said, even without these corrected and drastically reduced estimates, the official deaths attributed to COVID-19 have until recently failed to register in the European monitoring of excess mortality for public health action, which in week 12, ending 20 March, reported ‘normal or below-average’ mortality rates in the 24 participating countries (below left). Only last week did it finally report ‘excess all-cause mortality overall’ driven by ‘particularly high excess mortality in some countries, primarily seen in the age group of 65 years and above’ (below right).

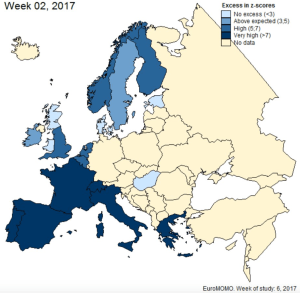
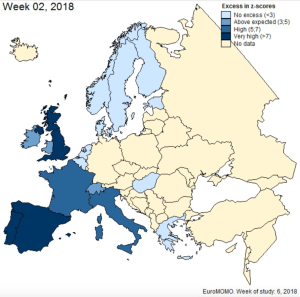
However, as has been pointed out in an article published anonymously — presumably for fear of reprisals — in Off-Guardian, even these exaggerated mortality rates are still far below the mortality rates in Europe at the height of the influenza waves over the winters of 2016-17 (below left) and 2017-18 (below right), during neither of which were the countries worst affected shut down by their governments.
5. The Media Virus
But what about the reports in the media about the number of deaths among doctors fighting the epidemic in Italy? Surely this is evidence of the seriousness of the coronavirus, and if it hasn’t killed as many people as officially reported, then isn’t that due to their heroic efforts, which have cost them their very lives?
Well, yes, it has been widely reported in the media that over 50 Italian doctors have died fighting the coronavirus, and cited as evidence of the seriousness of the threat of COVID-19. The National Federation of Orders of Surgeons and Doctors has even listed their names under the title ‘Doctors who died during the Covid-19 epidemic’, calling their deaths ‘a warning, a lesson for everyone’.
But let’s stop there and make sure we learn the right lesson. A look at the birth dates and medical specialisms of the deceased reveals that, of the 63 doctors who had died by 30 March, 40 were over the Italian retirement age of 67. The two youngest were both 48; 3 were in their 50s; 31 were in their 60s; 17 in their 70s; 5 in their 80s, 2 in their 90s; and the ages of 2 more were unidentified. They include 4 dentists aged 48, 65, 68 and 68; a 61 year-old sports physician; a 70 year-old ophthalmologist; a 73 year-old child neuropsychiatrist; an 86 year-old psychiatrist; and a 93 year-old paediatrician. With all due respect to their professions and their deaths, this doesn’t look like the frontline of doctors fighting the annual increase in deaths among over 65s in Northern Italy. Incredibly, given the context, this webpage doesn’t identify the actual causes of death, but it does at least admit that many of the doctor’s deaths were ‘not directly attributable to the virus’.
Undoubtedly, some of these medical professionals died through the increased exposure to SARs-CoV-19 consequent upon their attempts to limit its threat to the increased mortality rates of the over 70s — a struggle made all the harder by lack of resources available to the Italian health service; but this is not an accurate record of those deaths. On the contrary, it is another example of the deliberately false and inaccurate reporting about this manufactured crisis designed to spread panic and justify repressive government measures.
As further evidence of this intention, since I recorded the age of the doctors at death, The National Federation of Orders of Surgeons and Doctors has increased the number of doctors on their webpage to 71 — including a gynaecologist — but has now removed all their birth dates. So, for the record — and to pay them the respect they deserve for a lifetime’s service to medicine rather than trying to turn their deaths into a political tool — here are the ages of the 61 doctors for whom birth dates were provided a few days ago: 48, 48, 55, 56, 59, 61, 62, 62, 63, 64, 64, 65, 65, 65, 65, 65, 66, 66, 66, 66, 67, 67, 67, 67, 68, 68, 68, 68, 68, 69, 69, 69, 69, 69, 69, 69, 71, 71, 71, 72, 73, 73, 73, 73, 74, 74, 74, 74, 75, 76, 78, 78, 79, 80, 82, 82, 86, 89, 90 and 93.
6. The Emperor’s New Clothes
But, you might say, grasping at the final straw of the Government’s argument for suspending our civil liberties, isn’t this evidence of a lack of an epidemic because the governments of Italy and the UK have locked down their respective countries? Isn’t this proof of the correctness of this policy, and all the more reason why we should be obeying our Government’s instructions?
Well, let’s look at the alternatives. Despite intense international pressure, the governments of Sweden and Iceland, like those of Japan and South Korea, have not adopted the ‘lockdown’ strategies of Italy, Greece, Serbia, Slovenia, Romania, Austria, Hungary, the Czech Republic, Germany, Poland, Ukraine, Russia, Finland, Norway, Denmark, the Netherlands, Belgium, France, Spain, Portugal, Ireland and the UK, but have instead adopted the more rational and scientifically justified precaution of protecting the vulnerable — the elderly and those with pre-existing health conditions — and quarantining those who test positive for SARs-CoV-2. The results, according to the official figures, are that Sweden, with a population of 10.36 million, has 333 deaths linked to COVID-19; Iceland, as we have seen, with a population of 340,000 has 4, South Korea — where over 420,000 people have been tested, the highest per capita in the world — with a population of 51.27 million has 174; and Japan, with 126.5 million, has 63. Where are the 250,000 deaths that we were threatened with by our government should we adopt similarly rational measures? Where are the lines of hearses and photographs of over-filled hospitals with which we are inundated every day by our press and media?
I am not going to comment on the benign presence of corona viruses that have been present in our bodies for decades and infect tens of millions of people across the world every year. Or about the fact that corona viruses make up 5-14 per cent of all influenza viruses, and that if we tested every one of the 290,000 to 650,000 people that die every year of seasonal influenza, in the way that we are testing the hospitalised and deceased now, we would expect to find between 14,500 and 91,000 of them dying with coronavirus. I am neither a doctor nor an epidemiologist, so although I can quote these facts I don’t understand them enough to argue them; but there are plenty of epidemiologists, virologists, microbiologists and pulmonologists — and some of the most respected in the world — who do understand them, and have spoken up to criticise the way the media is creating panic out of COVID-19, and to condemn the suspension of civil liberties governments have imposed on the back of that panic. These include:
- Dr. Sucharit Bhakdi, Professor Emeritus of Medical Microbiology who served for 22 years as Chairman of the Institute of Medical Microbiology and Hygiene at the Johannes Gutenberg University Mainz and is one of the most cited research scientists in German history, who has written on open letter to the German Chancellor, Angela Merkel, criticising the measures she has imposed, which he has described in an interview as ‘grotesque, absurd and very dangerous’;
- Dr. John P.A. Ioannidis, Professor of Medicine, of Health Research and Policy and of Biomedical Data Science at the Stanford University School of Medicine, whose 2005 paper ‘Why Most Published Research Findings Are False’ is the most downloaded paper in the Public Library of Science, who has called our reaction to the coronavirus a ‘once-in-a-century evidence fiasco’;
- Professor Peter C. Gøtzsche, a physician, medical researcher, founder of the prestigious Cochrane Medical Collaboration and outspoken critic of the pharmaceutical industry, who has called the coronavirus ‘an epidemic of mass panic’.
- Dr. Knut Wittkowski, Head of the Department of Biostatistics, Epidemiology and Research Design at the Rockefeller University for 20 years, and who has been an epidemiologist modelling epidemics for 35 years, who in an interview has said that staying indoors under lockdown ‘keeps the virus healthy’, because ‘going outdoors is what stops every respiratory disease’.
- Dr. David L. Katz, President of the True Health Initiative and the founding director of the Yale-Griffin Prevention Research Center, who says he is ‘deeply concerned’ about the lockdown of society, the consequences of which could be ‘calamitous, possibly graver than the direct toll of the virus itself’.
- Dr. John Lee, Professor Emeritus of Pathology at Hull York Medical School and a former NHS consultant pathologist, who writes that we have ‘decided on policies of extraordinary magnitude without concrete evidence of excess harm’.
- Dr. John Oxford, Professor Emeritus of Virology at Queen Mary University London, one of the world’s leading virologists and influenza specialists, who has described the coronavirus as ‘akin to a bad winter influenza epidemic’, and concludes that ‘We are suffering from a media epidemic!’
- Dr. Wolfgang Wodarg, an epidemiologist specialising in pulmonology and the former chairman of the Parliamentary Assembly of the Council of Europe, who has compared the pandemic to the Hans Christian Andersen story about The Emperor’s New Clothes, except that the invisible clothes we are all pretending to see, he says, is a crown — coronavirus.
There are many more such expert testimonies, and we have a duty to what’s left of our citizenship to read every one of them, rather than relying for our knowledge and opinions on governments and their media outlets. Unfortunately, but entirely predictably, Government policy in the UK is being corroborated by our Chief Medical Officer for England since October 2019, when he was appointed by Conservative Prime Minister Boris Johnson, Professor Chris Whitty, who since 2015 has been a Companion of the Most Honourable Order of the Bath, the fourth-most senior of the British Orders of Chivalry; and by our Chief Scientific Advisor to the government since March 2018, when he was appointed by Conservative Prime Minister Theresa May, Sir Patrick Vallance, who in 2006 joined the multinational pharmaceutical company GlaxoSmithKline, one of the largest, most predatory, most prosecuted and most fined of the so-called ‘Big-Pharma’ corporations, which specialises in respiratory products and vaccines, and who between 2012-2018 was President of its Research and Development.
In my earlier article, Sociology of a Disease, I wrote about how Sir Patrick deliberately quoted figures on the average annual deaths from influenza in the UK (8,000) that were five years out of date and less than half more recent estimates (17,000) in order to exaggerate the already exaggerated estimates of the death-toll from COVID-19 (250,000-510,000) if we didn’t obey the government’s suspension of our civil liberties (in which case he estimated 20,000). But to get an idea of how embedded these two figures are in the British establishment, listen to Sir Patrick concede to the recent suggestion by Jeremy Hunt MP, the former Health Secretary perhaps most responsible for dismantling and privatising the National Health Service, that ‘saving lives’ from the coronavirus justifies tracking the mobile phones of everyone in the UK.
To believe that these two figures are in any way impartial or independent of the Government is like believing that the British press that has lied to us about the perpetrators of 9/11, about the existence of weapons of mass destruction in Iraq, about the justification for the so-called war on terror, about UK arms deals to Saudi Arabia, about the causes of and solutions to the financial crisis, about the justifications for fiscal austerity, about the extent of the privatisation of the NHS, about the detention and arrest of Julian Assange, about the arrest and imprisonment of Chelsea Manning, about who was responsible for the Grenfell Tower fire, about the 16 months of protests by the Gilets jaunes, about the supposed anti-semitism of Jeremy Corbyn, about the causes and solutions to the housing crisis, about the causes and solutions to the environmental crisis — about every major event, in other words, of the past twenty years and longer — is suddenly telling the truth about the coronavirus. Unfortunately, the vast majority of the British people have done just that.
I can only hope, therefore, that in addition to the testimonies of senior and respected medical specialists from around the world who are independent and critical of the actions of their governments, the analysis of the facts and figures about SARs-CoV-2 presented in this article will convince its readers that there is no coronavirus pandemic. There is certainly no increase in deaths even suggesting a viral epidemic in the UK. In certain areas of Europe, such as Northern Italy, Spain and the North-east of France — due to a combination of high pollution levels, an ageing population, shortages of staff and equipment for underfunded health services compounded by government policy that is, for instance, cancelling medical tests and operations for the elderly and sick and sending all staff home that test positive for SARs-CoV-2 irrespective of whether they develop symptoms, thereby further depleting the level of health care — there is a higher mortality rate among over 65s. But across the rest of Europe the usual number of people within the usual age range and health profile are dying at the usual rate from a new but in no respect more infectious or more fatal virus than those that cause seasonal influenza every year, often with far higher rates of mortality, including the children who so far appear largely resistant to COVID-19. But what is new — what is completely unprecedented and should be the cause of alarm and action — is how the governments of most European countries are reacting to it.
Presumably because of some or all of these reasons, on 19 March, Public Health England removed COVID-19 from the list of high consequence infectious diseases (HCID) in the UK. The definition of an HCID is that it is an acute infectious disease; typically with a high rate of case to fatality; which may not have effective prevention or treatment; is often difficult to recognise and detect rapidly; has the ability to spread in the community and within healthcare settings; and requires an enhanced individual, population and system response to ensure it is managed effectively, efficiently and safely. The main reason cited for this downgrading of COVID-19 from its initial categorisation in January 2020 as an HCID is the new information about its mortality rates, which are now cited as ‘low overall’. So why, a week later, did the UK Parliament pass the Coronavirus Act 2020 suspending many of our human rights for the next two years, and the Secretary of State for Health, without scrutiny or approval by Parliament, make the Health Protection (Coronavirus, Restrictions) (England) Regulations 2020 enforceable by the police and radically constraining our civil liberties for the next 6 months?
In Part 2 of this article I’ll be looking at the consequences for us, already and in the future, of our collective readiness to see the invisible clothes of our new king, and of our failure, individually, to point at the British government and accuse it of turning this media-manufactured crisis to its own political ends.
Further reading:
The Science and Law of Refusing to Wear Masks: Texts and Arguments in Support of Civil Disobedience
Lockdown: Collateral Damage in the War on COVID-19
Manufacturing Consensus: The Registering of COVID-19 Deaths in the UK
Giorgio Agamben and the Bio-Politics of COVID-19
Good Morning, Coronazombies! Diary of a Bio-political Crisis Event
Coronazombies! Infection and Denial in the United Kingdom
Sociology of a Disease: Age, Class and Mortality in the Coronavirus Pandemic
Simon Elmer
Architects for Social Housing
Architects for Social Housing is a Community Interest Company (no. 10383452). Although we occasionally receive minimal fees for our design work, the majority of what we do is unpaid and we have no source of public funding. If you would like to support our work financially, please make a donation through PayPal:
![]()

3 thoughts on “Language is a Virus: SARs-CoV-2 and the Science of Political Control”