
Table of Contents
Part 2. Virtue and Terror
-
- Censorship and Consent
- How to ‘Vaccinate’ UK Children
- Virtue and Terror
- Crime and Punishment in the UK Biosecurity State
1. Censorship and Consent
On 9 February, 2021, Luke Garrett, a 20-year-old Scottish man with muscular dystrophy and autism but otherwise fit and well, died less than 12 hours after being injected with the messenger RNA Pfizer ‘vaccine’. Mr. Garrett, who had been shielding for a year, had been eagerly waiting for the ‘vaccine’, he said, so that he could resume his life. Injected at 3pm the previous day, he almost immediately developed a high temperature followed by severe muscle pain, particularly in the injected arm. Mr. Garrett then went into a seizure, which he had never had before, and began foaming at the mouth. His mother performed CPR (cardiopulmonary resuscitation) on him until the paramedics arrived after 1am and gave him an adrenaline shot, before promising additional medical care would arrive in two hours. At 4am, when the hospital rang to ask whether he still needed help, Luke Garrett was dead. In response, an unidentified Scottish Government spokesman said:
‘The vaccines are safe and approved by regulators — including the MHRA — and we encourage all those who are offered to get vaccinated. No causal link has been made between the Pfizer vaccine and any fatality in the UK. The MHRA is alerted of all deaths where a patient was recently vaccinated and they will draw their own conclusions. It would be inappropriate to comment further on any individual case.’
The Medicines and Healthcare products Regulatory Agency said:
‘The current evidence does not indicate an association between the COVID-19 vaccines and onset of seizure events in people with or without a prior history of seizure.’
Dr. Joy Tomlinson, Joint Director of Public Health at NHS Ayrshire and Arran, where the Ballochmyle Medical Practice had administered the ‘vaccine’, said:
‘We continue to urge those offered a vaccination to take up their appointment. The benefits of the COVID-19 vaccines outweigh the risks and it continues to be a safe and effective vaccine.’
Pfizer, the pharmaceutical company that manufactures the ‘vaccine’, said:
‘We take adverse event reports very seriously. To date, millions of people have been vaccinated with our vaccine. It is important to note that serious adverse events can occur in the population that may be unrelated to the vaccine.’
Finally, Muscular Dystrophy UK said:
‘The MHRA has confirmed to us that their analysis of data relating to people who have received a Covid-19 vaccine has not shown any linkage between having a muscle-wasting condition and experiencing vaccine side-effects. We are not clinically trained ourselves, so rely on collaborations with leading neuromuscular clinical and healthcare professionals to help us to provide the information and advice to do this.’
At any other time, this blanket denial of any causal connection between the death of this young man and an experimental ‘vaccine’ by the pharmaceutical company that produced it, the medical practice that administered it, the charity that recommended it, the regulatory agency that authorised it, and the government pushing it as part of the UK ‘vaccination’ programme, would be extraordinary, unbelievable, sinister and worthy of investigation. In the UK biosecurity state built on the justification of this manufactured crisis, it’s now the New Normal.
For publishing the figures on adverse drug reactions and deaths following injection with a COVID-19 ‘vaccine’ that I discussed in Part 1 of this article — all of which were either quoted directly from the Medicines and Health products Regulatory Agency’s own website or calculated from the Government’s own estimation of the percentage of ADRs reported — my account was temporarily suspended by Twitter for what it said was ‘spreading misleading and potentially harmful information related to COVID-19.’ In addition to this suspension, my post was removed because, Twitter claimed, it included ‘content that goes directly against guidance from authoritative sources of global and local public health information’. For information on COVID-19, Twitter directed me to a World Health Organisation webpage containing ‘advice for the public’.
Now, anyone who dares to question the orthodoxies of the UK biosecurity state has come to expect the enforcement of a level of censorship we wouldn’t believe was possible in this country 18 months ago; and most of us have experienced something similar to this or far worse by now, so I don’t want to dramatise its impact. Initially, I appealed the decision, but after a week I’d received no response from Twitter and decided to accept the removal of this post; then, as soon as my account was restored to activity in a further 12 hours, I updated the figures from the most recent MHRA information and reposted it. But neither do I want to normalise what is an interference not only with my individual freedom of expression and conscience, both of which are protected under the European Convention on Human Rights (ECHR), but also — and more seriously within the context of the UK ‘vaccination’ programme — a breach of one of the conditions of any medical treatment, which is the informed consent of the person being treated. In this section, I want to look at the requirements of consent under international and UK law and medical practice, and show how the UK ‘vaccination’ programme has manufactured the consent of the UK public through censorship of the information by which those requirements can be met.
Let’s start with the Nuremberg Code, which was published in 1947 following the Nuremberg Trial of medical doctors indicted for crimes against humanity during the 12 years of the Third Reich, and in doing so established new standards of ethical behaviour to which professionals conducting medical experiments are expected to adhere. It is mere sophistry to suggest, as the consistently pro-biosecurity website FullFact has done, that the Nuremberg Code does not apply to the UK ‘vaccination’ programme because it is not experimental. First, the clinical trials for the AstraZeneca viral-vector ‘vaccine’ won’t be completed until February 2023, until May 2023 for the mRNA Pfizer ‘vaccine’, and until October 2022 for the mRNA Moderna ‘vaccine’. Second, as experimental ‘vaccines’, they have only been granted temporary authorisation by the MHRA under The Human Medicines (Coronavirus and Influenza) (Amendment) Regulations 2020, in which the newly-introduced Regulation 174a modified The Human Medicines Regulations 2012 to allow temporary authorisation of the supply of unlicensed medicines, including COVID-19 vaccines, in response to certain threats to public health. Third, although tested on human subjects for several infectious diseases including rabies and influenza, the messenger RNA bio-technology employed in the Pfizer/BioNTech and Moderna/NIH ‘vaccines’ has never before been authorised for emergency use on humans as part of a mass ‘vaccination’ programme. Finally, as I laid out in Part 1 of this article, both the documented record and estimated number of adverse drug reactions and deaths following injection with these ‘vaccines’ are out of all proportion to previously-issued vaccines, and clearly indicate their experimental and, indeed, dangerous nature. Given which, the ethical principles of the Nuremberg Code cannot be so easily dismissed — as so many questions and objections to the UK ‘vaccination’ programme have been dismissed — by ‘Fact Check’ claims by tech companies, news outlets and social media sites according themselves the right to tell us what we can and cannot read, what is and isn’t true.
The most important standard of the Nuremberg Code, and the one most violated by the UK ‘vaccination’ programme, is the first, which states:
‘The voluntary consent of the human subject is absolutely essential. This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, overreaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment.
‘The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs, or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.’
It is by now a matter of public record that, in the UK as in every other country that has imposed coronavirus-justified restrictions on the population, the ‘vaccination’ programme has violated the conditions under which voluntary consent can be given: through daily misinformation about the threat of COVID-19 to public health and therefore about the necessity of being ‘vaccinated’, through the censorship of information about the level of risk and danger to health of being ‘vaccinated’, and through making compliance with this programme a condition of our freedoms, and in doing so of exerting coercion over the free choice of the individual to choose to participate in this experimental ‘vaccine’ programme.
However, even if we accept claims by the pharmaceutical companies producing them, the media companies promoting them and the medical institutions administering them, that the UK ‘vaccination’ programme is not experimental but has been authorised for temporary use by the UK Government, the same requirements for voluntary and informed consent apply to all medical treatment under UK and international law. It is representative of the way COVID-propagandists like Full Fact and other so-called ‘fact-checkers’ work that, by challenging the applicabilty of the Nuremberg Code to the UK ‘vaccination’ programme, they have ignored all the other legislation and codes of conduct that impose the same conditions of consent.
As I discussed in an earlier article that looked at Compulsory ‘Vaccination’ for COVID-19 and Human Rights Law, the European Court of Human Rights has established that medical treatment without consent constitutes an interference with Article 8 of the ECHR, with case law (Pretty vs. United Kingdom, 2002) stating:
‘The imposition of medical treatment, without the consent of a mentally competent adult patient, would interfere with a person’s physical integrity in a manner capable of engaging the rights protected under Article 8(1) of the Convention.’
Since vaccination is defined as medical treatment under Section 45E of the Public Health (Control of Disease) Act 1984, compulsory ‘vaccination’ would constitute such interference for people who would otherwise refuse. It is in conformity with this legal requirement that the National Health Service has imposed three requirements for ‘consent to medical treatment’. These are that consent is:
-
- ‘Voluntary — the decision to either consent or not to consent to treatment must be made by the person, and must not be influenced by pressure from medical staff, friends or family;
- ‘Informed — the person must be given all of the information about what the treatment involves, including the benefits and risks, whether there are reasonable alternative treatments, and what will happen if treatment does not go ahead;
- ‘Capacity — the person must be capable of giving consent, which means they understand the information given to them and can use it to make an informed decision.’
The violation of these requirements opens anyone doing so, including a clinician, to criminal charges. Reviewing the legal barriers to compulsory medical intervention being considered by the Government last year, Rosalind English, a former lecturer on law and genetics at the University of Cambridge and part of the editorial team of the UK Human Rights Blog run by 1 Crown Office Row barristers’ chambers, wrote:
‘Vaccination without consent would be prohibited by the criminal law on assault, and even grievous bodily harm, if the consequences of the treatment are serious.’
As I documented in Part 1 of this article, the consequences of injection with COVID-19 ‘vaccines’ have been very serious and even fatal. One could propose, therefore, that anyone collaborating in overriding these conditions of consent was aiding and abetting in assault and possibly in grievous bodily harm.
By suspending my account, therefore, and removing my post publicising what these risks are based on the MHRA’s own figures, Twitter had in effect over-ruled the second condition of consent to COVID-19 ‘vaccination’: that those giving consent are first given all the information about what the treatment involves, including the benefits and risks of ‘vaccination’. Now, obviously, it is not from my Twitter account that the millions of UK citizens being pressured and coerced into being injected should go for their information; but neither is there any justification for censoring my contribution to sharing that information. Far more importantly, in reporting my post to Twitter, Public Health England had collaborated in the blanket censorship by the UK Government, media and medical profession of all the information about these COVID-19 ‘vaccines’, when it should, to the contrary, as the executive arm of the Department of Health and Social Care, be making this information available to each and every UK citizen in full and before they make the decision whether or not to be injected. It is not the job, the responsibility or the legal right of PHE to make that decision for us, and no unfounded claims about spreading information ‘harmful’ to the effectiveness of the UK ‘vaccination’ programme or dismissive allusions to ‘conspiracy theories’ should allow these public bodies to assume that right, in violation of the requirements of voluntary, informed and capable consent under UK law and NHS practice.
These accusations have been clearly and publicly stated in a letter dated 2 July, 2021, addressed to Simon Stevens, Chief Executive Officer of the NHS, by Philip Hyland, Principle at employment law solicitors, PJH Law, on behalf of Dr. Sam White. Dr. White is a General Practitioner and member of The International Lyme & Associated Disease Society whose license to practice medicine was suspended by the NHS on 16 June, 2021, for posting a video on his personal social media account in which he argued that:
‘The vaccine programme has been rolled out in breach of the legal requirements for clinicians to obtain the free and informed consent of those being vaccinated’.
This is an open letter, made available online, and I want to look at some of its accusations, which Dr. White makes not only against the Executive Board of the NHS, his former employer, but also against the UK Government, its Scientific Advisory Group for Emergencies, senior public office holders within the civil service, and the Executive Board of the Medicines and Health products Regulatory Agency. The letter starts with the statement that clinicians practicing within the NHS are obliged to do two things when administering any vaccine, and not just the COVID-19 ‘vaccines’:
-
- ‘To do no harm.
- ‘To obtain the free and informed consent of those being vaccinated.’
The first obligation derives from a slightly inaccurate Latin translation (‘primum non nocere’) of a text attributed to the Ancient Greek physician Hippocrates, and is one of the principal precepts of bioethics that all students in healthcare are taught in school. The second obligation, however, is not merely a principle but established by the Supreme Court (Montgomery v. Lanarkshire Health Board [2015] UKSC 11). As summarised in the letter, the principles of what constitutes free and informed consent are as follows:
-
- ‘That the patient is given sufficient information to allow individuals to make choices that will affect their health and well-being.
- ‘“Sufficient information” includes informing the patient of the availability of other treatments.
- ‘That the patient is informed of the material risks of both taking and declining the vaccine.’
As the letter also points out, these principles are in line with Article 6 of UNESCO’s Universal Declaration on Bioethics and Human Rights, according to which:
‘Any preventive, diagnostic and therapeutic medical intervention is only to be carried out with the prior, free and informed consent of the person concerned, based on adequate information.’
Breach of these principles, therefore, constitutes professional gross misconduct at an individual level; while at an organisational level, if the NHS does not produce evidence that every person injected with a COVID-19 ‘vaccine’ by its staff has been granted prior consent that meets these principles, NHS executives will — at least in principle — be legally liable for its institutional failings, notwithstanding the indemnity from liability conferred by Government changes to The Human Medicines Act.
The rest of the letter is taken up with laying out the failings of the NHS to meet these principles, which it divides into the following three categories:
-
- The inadequacy of the information made available to the public about the material risk of infection with SARS-CoV-2 and hospitalisation, dying or recovering from COVID-19.
- The inadequacy of the information made available to the public about the availability of other treatments to combat infection with SARS-CoV-2 and symptoms of COVID-19.
- The inadequacy of the information made available to the public about the risks of injection with a COVID-19 ‘vaccine’.
From this catalogue of failings — whose enumeration in this letter runs to more than 20 pages, and which I recommend to everyone as a summary of the duplicity of the medical response to the coronavirus crisis in the UK — these are the main accusations Dr. White makes against the Government, SAGE, MHRA and NHS.
- Failing to differentiate between positive RT-PCR or Lateral Flow antigen tests and individuals diagnosed by a doctor as either infected with SARS-CoV-2 or ill with COVID-19, as is required by the NHS’s own internal leaflet;
- Failing to distinguish between those patients admitted to hospital with symptoms of COVID-19, those who have subsequently tested positive and those who caught SARS-CoV-2 in hospital;
- Failing to differentiate between those who have died from COVID-19 and those who died from another medical condition but who tested positive either within 28 days prior to death or post-mortem;
- Failing to differentiate between the programme of immunisation presented to the UK public and the UK ‘vaccination’ programme whose clinical trials were exclusively for efficacy of symptom reduction, not for immunity from infection or reduction of transmission;
- Failing to explain and justify the changes in policy from ‘vaccinating’ the vulnerable, to ‘vaccinating’ a sufficient percentage of the UK population to achieve herd immunity, to mass ‘vaccination’ of the entire population, including children;
- Failing to make clear to those ‘vaccinated’ by NHS clinicians that the ‘vaccines’ are still undergoing clinical trials, have never been used on humans before as part of a vaccination programme, and that there is, therefore, no data on their long-term effects;
- Failing to make clear to those ‘vaccinated’ that the clinical trials were not conducted on pregnant women, the elderly or those who had already been infected with SARS-CoV-2, for none of whom, therefore, is there any data on the consequences for their health;
- Failing to make clear to those ‘vaccinated’ that the COVID-19 ‘vaccines’ are not licensed but have only been granted temporary authorisation by the MHRA, which is a lower regulatory threshold;
- Failing to differentiate between relative risk reduction (the difference between those developing symptoms of COVID-19 with and without a ‘vaccine’) which is 95 per cent in Pfizer, 94 per cent in Moderna and 67 per cent in AstraZeneca, and absolute risk reduction (the difference between those developing symptoms with and without a vaccine among the whole population), which is 0.84 per cent for Pfizer, 1.2 per cent for Moderna and 1.3 per cent for AstraZeneca);
- Failing to call out and distance itself from celebrities paid to advertise and promote COVID-19 ‘vaccines’ that have not received marketing authorisation from the MHRA, and which is therefore in contravention of The Human Medicines Regulations 2012.
- Failing to call out and distance itself from unlawful coercion by the Government in making ‘vaccination’, and proof of ‘vaccination’ in the form of ‘vaccine’ passports, a condition of, for example, removing lockdown restrictions, gaining access to certain venues or permitting travel to holiday destinations. This use of coercion, which is endemic in the UK ‘vaccination’ programme, is in contravention of the Council of Europe’s Resolution 2361 on ‘Covid-19 vaccines: ethical, legal and practical considerations’. Adopted by the Parliamentary Assembly on 21 January this year, this states that Member states, which include the UK, must:
‘7.3.1. ensure that citizens are informed that the vaccination is not mandatory and that no one is under political, social or other pressure to be vaccinated if they do not wish to do so;
‘7.3.2. ensure that no one is discriminated against for not having been vaccinated, due to possible health risks or not wanting to be vaccinated.’
- Failing to make it clear to the public that the NHS does not endorse the fettering of an individual’s right to either consent to or decline any medical intervention;
- Failing to publish information about the effectiveness of the human immune system, and how it can be enhanced by vitamin D, in fighting off infection and disease; the superiority of human antibodies and the longevity of T and B cells in providing immunity over the protection afforded by ‘vaccines’, and the availability and success of other treatments, including Ivermectin, Zinc and Budoneside anti-inflammatory inhalers, in treating the symptoms of COVID-19;
- Failing to inform the public of the risks to the health of those injected with these temporarily-authorised ‘vaccines’, including failing to publish and disseminate the data on adverse drug reactions following injection, which include Bell’s palsy, thrombo-embolic events with concurrent low platelets, Capillary Leak Syndrome, menstrual disorders and unexpected vaginal bleeding, myocarditis and pericarditis, Guillain-Barré Syndrome, antibody dependant enhancement and, in certain cases, death;
- Failing to collate or publish data on deaths within 28 days of injection with COVID-19 ‘vaccines’.
For all of these failings and others, Dr. White argues that the National Health Service has failed to provide the UK public with the information it needs to meet the requirements of informed consent under UK law and NHS best practice, and is, therefore, in breach of its obligations to the UK public. Additionally, by actively censoring this information, the UK Government has turned NHS clinicians into ‘conduits’ for Government policy, and are therefore guilty of ‘politicising health’, which it is his duty as a medical professional to call out. ‘Clinicians’, Dr. White argues, ‘should feel able to voice genuine concerns relating to alleged malpractice without fear for their ability to practice within the NHS being suspended.’ Undoubtedly they should; but in the UK biosecurity state in which we now live, for fulfilling his own obligations to the UK public and refusing to administer the UK ‘vaccination’ programme without the voluntary and informed consent of patients capable of granting it, Dr. White continues to be suspended from medical practice by the NHS. The letter from his lawyers concludes:
‘The issues raised by my client and other clinicians who have not been suspended raise issues about the integrity of those leading the Covid response. They raise issues about whether the information that has been provided to the public has been collected and presented fairly. They raise issues of breaches of the law and accepted standards in public life. They raise issues of whether private individuals with charitable foundations have too much influence on policy direction and whether the financial support offered by those individuals and foundations is healthy in a transparent democracy.’
‘By endorsing the vaccine passport policy the National Health Service is not only endorsing a breach of international law which makes sacrosanct an individual’s right to decline any medical intervention without any repercussion but also breaches the UK law on informed consent. Since when did the National Health Service morph into the National Pharmaceutical Distribution Service?’
2. How to ‘Vaccinate’ UK Children
On 13 June, Jacob Clynick, a 13-year-old boy from the USA with no pre-existing medical conditions, was injected with his second dose of the Pfizer ‘vaccine’. Over the next two days he felt tired and developed a fever, and on the evening of 15 June he had a stomach-ache. Retiring early, Jacob never woke up, having died in his sleep in the early hours of 16 June. The family were told that findings from the preliminary autopsy suggested his heart was enlarged when he died, and that there was fluid around his heart. No cause of death was listed on Jacob’s death certificate. On 23 June, three days before Jacob’s funeral, the Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices admitted there was a ‘likely association’ between ‘vaccines’ employing the experimental messenger RNA biotechnology and myocarditis and pericarditis. Myocarditis is the inflammation of the heart muscle that can affect heart rhythm and its ability to pump, while pericarditis is the inflammation of the sac around the heart, and both have been more prevalent in boys and young men following injection with a COVID-19 ‘vaccine’. According to the Vaccine Adverse Event Reporting System (VAERS), the US equivalent of the MHRA, as of 27 August there have been 586 reports of 12-15-year-old children hospitalised in the US, including 9 who have died, following injection with a COVID-19 ‘vaccine’. Two weeks ago, on 8 September, a US study, ‘SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17’, reported that, between 1 January and 18 June, 2021, boys aged 12-15 with no underlying medical conditions were 3.7-6.1 times more likely to be diagnosed with myocarditis after two doses of mRNA ‘vaccines’ — with 86 per cent requiring hospital care — than they were of ending up in hospital with COVID-19. As of 15 September, the CDC has confirmed 890 reports of myocarditis or pericarditis in male adolescents and young adults following injection with mRNA ‘vaccines’.
Back in the UK, as of 8 September, 2021, the MHRA has received 275 reports of myocarditis and 205 reports of pericarditis following injection with the Pfizer ‘vaccine’ that killed Jacob Clynick. Including injection with the Moderna ‘vaccine’, which employs the same mRNA bio-technology, and the viral vector AstraZeneca ‘vaccine’, there have a total of 433 reports of inflammation of myocarditis and 407 reports of pericarditis. The MHRA comments:
‘There has been a recent increase in reporting of these events in particular with the Pfizer/BioNTech and Moderna vaccines, with a consistent pattern of cases occurring more frequently in young males and shortly after the second dose of the vaccines.’
At a recent conference panel on parental consent to COVID-19 vaccines, Dr. Tony Hinton, an Ear, Nose and Throat Consultant Surgeon at New Victoria Hospital in Kingston-upon-Thames, said that 1 in 6,000 young people aged 12-24 develop myocarditis following injection with a COVID-19 ’vaccine’; that 50 per cent with myocarditis die within 5 years; that males are ten times more likely to develop myocarditis than females; and that ten times more die after a second injection.
In this next section, I want to look at how the Government has extended the UK ‘vaccination’ programme to these children, when they are even less capable of meeting the legal requirements and practical definition of consent to medical treatment under UK law. In the last section I quoted the first standard of the Nuremberg Code, laying out the conditions under which consent can be said to be voluntary and informed; but there are, in addition, two other standards relevant to the UK ‘vaccination’ programme, and in particular to its imminent extension to children between 12 and 15 years old. These are standards 5 and 6, which require that:
-
- ‘No experiment should be conducted where there is an a-priori reason to believe that death or disabling injury will occur.
- ‘The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.’
I’ll come back to why the UK ‘vaccination’ programme fails to meet both these standards; but in addition to being a signatory of the Nuremberg Code, the UK Government is also beholden to the United Nations Convention on the Rights of the Child, which it ratified in December 1991. These include the following rights (which I quote from both the full convention and its summary) most relevant to the extension of the UK ‘vaccination’ programme to children:
‘Article 3. In all actions concerning children, whether undertaken by public or private social welfare institutions, courts of law, administrative authorities or legislative bodies, the best interests of the child shall be a primary consideration.’
‘Article 6. Every child has the right to life. Governments must do all they can to ensure that children survive and develop to their full potential.’
‘Article 17. Ensure that the child has access to information and material from a diversity of national and international sources, especially those aimed at the promotion of his or her social, spiritual and moral well-being and physical and mental health.’
‘Article 36. Governments must protect children from all other forms of exploitation, for example the exploitation of children for political activities, by the media or for medical research.’
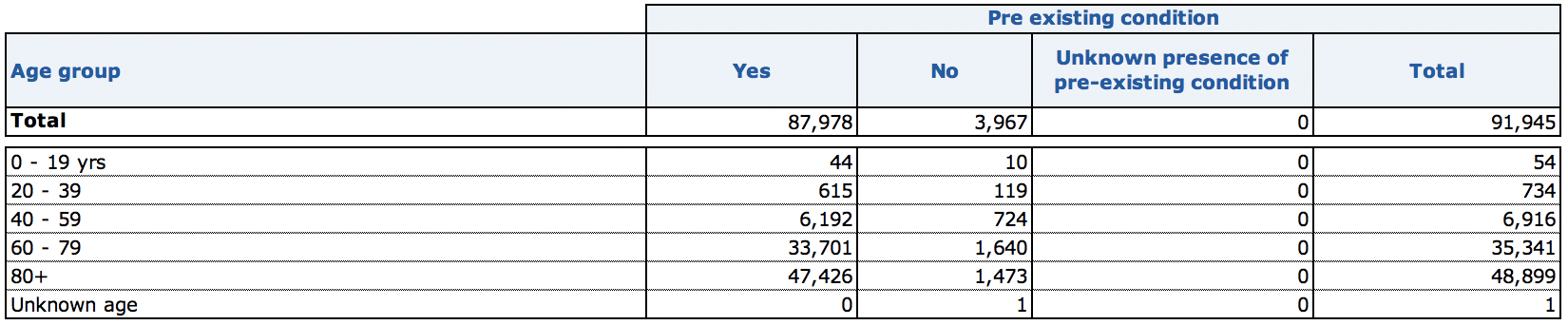
According to the most recently published figures by the Office for National Statistics, between the week ending 13 March, 2020, when the first deaths in the UK were attributed to COVID-19, and 14 September, 2021, 2,019 children between the ages of 1 and 19 died in the UK (I haven’t included the 3,566 deaths of infants under the age of 1, as this would distort the proportions). Of these, the ONS has recorded 46 deaths that ‘involved’ COVID-19 (with an additional 4 deaths under the age of 1 also recorded). According to the criteria by which COVID-19 deaths are recorded, therefore, 18 months into a supposed ‘pandemic’ the disease has been involved in 2.27 per cent of all child deaths in the UK. The real figures, however, are even worse than that, if by worse we mean justifying extending the UK ‘vaccination’ programme to children. According to the most recent NHS records (below), as of 15 September, 2021, only 10 children without a previously-existing health condition have had their deaths attributed to COVID-19 in hospitals in England and Wales since the pandemic began.
In addition to this UK data showing the almost total absence of threat COVID-19 presents to the health and lives of British children, the growing data from the US and other countries in advance of the UK in injecting their children with COVID-19 ‘vaccines’ and showing the greatly increased risk of myocarditis and pericarditis in ‘vaccinated’ children and young adults, added to the tiny absolute risk reduction of developing symptoms of COVID-19 these ‘vaccines’ actually confer, provides strong evidence for concluding that:
- Contrary to Article 3 of the UN Conventions on the Right of the Child, ‘the best interests of the child’ are not a primary consideration in the UK ‘vaccination’ programme;
- Contrary to Article 6, the UK Government is not doing all it can do ‘to ensure that children survive and develop to their full potential’;
- Contrary to Article 17 and 36, the UK Government is not promoting the ‘physical and mental health’ of our children or protecting them from ‘exploitation’ for ‘medical research’;
- Contrary to Standard 5 of the Nuremberg Code, there is ‘reason to believe that death or disabling injury will occur’ following ‘vaccination’;
- Contrary to Standard 6 of the Nuremberg Code, the ‘degree of risk’ of injury or death outweighs the purported ‘humanitarian importance’ of injecting our children with these experimental and dangerous drugs, about whose long-term consequences we know almost nothing, but whose immediate dangers to the health of those on whom they are being tested are becoming more apparent with each child that falls ill or dies following injection.
In support of this conclusion, on 3 September the Joint Committee on Vaccination and Immunisation (JCVI), citing ‘evidence of an association between mRNA COVID-19 vaccines and myocarditis’, released a statement in which they concluded that ‘the margin of benefit is considered too small to support universal vaccination of healthy 12 to 15 year olds’. Initially, this appeared to have undermined the Government’s plans to inject UK children under 16 with the Pfizer/BioNTech ‘vaccine’. However, there is another right in the UN Convention on the Rights of the Child relevant to the ‘vaccination’ of 12-15-year-old children, and that is Article 12, which states:
‘Article 12. State parties shall assure to the child who is capable of forming his or her own views the right to express those views freely in all matters affecting the child, the views of the child being given due weight in accordance with the age and maturity of the child.’
Two days later, on 5 September, Nadhim Zahawi, at the time the Parliamentary Undersecretary of State for COVID-19 Vaccine Deployment but since promoted to Secretary of State for Education, announced that children under the age of 16 will not be required to gain parental consent before being injected with a ‘vaccine’. According to a document published by the NHS just three weeks earlier, on 13 August, titled ‘COVID-19 vaccination programme: Vaccinating children and young people: frequently asked questions’, children can choose to be injected with the Pfizer/BioNTech ‘vaccine’ if they are ‘Gillick competent’. Established by the case of Gillick v West Norfolk and Wisbech Area Health Authority [1985] UKHL7 in order to allow doctors to prescribe contraceptives, treat STDs or perform an abortion on teenagers without the consent of their parents, this definition, according to NHS guidelines on ‘Children and young people: consent to treatment’, means that:
‘Children under the age of 16 can consent to their own treatment if they’re believed to have enough intelligence, competence and understanding to fully appreciate what’s involved in their treatment. This is known as being Gillick competent.’
Finally, on 13 September, the Chief Medical Officers of England, Scotland, Wales and Northern Ireland published a collective statement announcing that they were overriding the advice of the JCVI and authorising the injection of 3.15 million 12-15-year-old UK children with one dose of the Pfizer/BioNTech experimental mRNA ‘vaccine’. How they justified this medically, when both Pfizer and BioNTech have released their own statement that phase 3 of the clinical trials of its ‘vaccine’ only evaluated the safety and efficacy of a 2-dose schedule separated by 21 days, the CMOs didn’t say. But, contrary to the data showing that schools are not a site of asymptomatic transmission from children to adults, their justification for this decision was that the risk the ‘vaccines’ present to the health of UK children, including their deaths, is outweighed by being able to ‘maintain children and young people in secondary school and minimise further education disruption’. Besides the duplicity of citing the benefits of being able to remove a barrier to attending school that the UK Government, on the advice of the CEOs, is responsible for erecting, and the criminal disregard for the health and even the lives of UK children, this justification violates every condition, requirement, standard and law of voluntary consent I have quoted in this article.
Two days later, on 15 September, the National Health Service sent out a letter to all GP practices, all COVID-19 ‘vaccination’ sites and centres, all directors of public health and children’s services, all NHS trust CEOs and regional directors, and all local authority executives, informing them that, following the acceptance by the Secretary of State for Health and Social Care of the recommendation of the CEOs to ‘vaccinate’ UK children aged 12-15, providers should liaise with schools to send out ‘consenting leaflets’ to the parents and carers of these children to agree a date for ‘vaccination’, and should ensure that the ‘consent processes follows best practice outlined in the Green Book’. Published in June 2021, chapter 2, titled ‘Consent’, states:
‘For consent to immunisation to be valid, it must be given freely, voluntarily and without coercion by an appropriately informed person who has the mental capacity to consent to the administration of the vaccines in question. This will be the person themselves, someone with parental responsibility for an individual under the age of 18 years (16 years in Scotland), someone authorised to do so under a Lasting Power of Attorney (LPA) for health and welfare, or someone who has the authority to make treatment decisions as a court appointed deputy.’
For children under 18, however, consent relies on their being Gillick competent:
‘Where someone aged 16 or 17 years consents to vaccination, a parent cannot override that consent. Young people who understand fully what is involved in the proposed procedure (referred to as ‘Gillick competent’) can also give consent, although ideally their parents will be involved. If a Gillick-competent child consents to treatment, a parent cannot override that consent.’
On what constitutes Gillick competence, the Green Book refers to the criteria used by the National Society for the Prevention of Cruelty to Children (NSPCC). These criteria assess:
-
- ‘The child’s age, maturity and mental capacity;
- ‘Their understanding of the issue and what it involves — including advantages, disadvantages and potential long-term impact;
- ‘Their understanding of the risks, implications and consequences that may arise from their decision;
- ‘How well they understand any advice or information they have been given;
- ‘Their understanding of any alternative options, if available;
- ‘Their ability to explain a rationale around their reasoning and decision making.’
What neither the Government nor the NHS has explained is how this assessment is to be conducted on 3.15 million children between the age of 12-15 in the single week before commencement of the ‘vaccination’ programme no later than 22 September, the date on which I publish this article. What this will mean in practice is that, over the next month, children who under UK law are too young to make the decision to smoke, drink alcohol, consent to sex, rent or buy age-rated films, get a tattoo or piercing, work full-time, drive a car, change their name, open a bank account, serve on a jury or vote in an election, who have been subjected to 18 months of coronavirus-justified restrictions in school and at home, to campaigns of guilt and blame in the media about them ‘killing granny’, to lies from the Government about the level of threat of COVID-19 to themselves and others, to indoctrination by their teachers into the cultic practices of biosecurity, to peer pressure from their fellow schoolchildren to comply with the New Normal, and with totally inadequate and misleading information about the risks and possible consequences for them of being injected with these experimental ‘vaccines’ for a disease to which they are statistically immune — will nonetheless be classified as Gillick competent to overrule their parents. Presumably, this represents the less than ‘ideal’ circumstances under which their parents cannot override their decision.
Finally, this week the UK Health Security Agency, the newly-formed merger of Public Health England, NHS Track and Trace and the Joint Biosecurity Centre, published the ‘Coronavirus vaccine consent form for children and young people’, which confirmed my fears about the disinformation and lack of information provided to children before ‘vaccination’. I’ll briefly point out here the more glaring inadequacies and inaccuracies in the 2 pages and 18 sentences on whose understanding 12-15-year-old children are to be judged as Gillick competent to make this irreversible decision.
- ‘Coronavirus is an illness that lots of people are catching at the moment.’ In fact, coronavirus is not an illness (COVID-19) but a virus (SARS-CoV-2) that can, in a small percentage of those infected, develop into symptoms. This isn’t merely a distinction of terminology, but a product of how a positive RT-PCR test continues, against all the scientific evidence, to be equated with disease symptoms. Far from lots of people catching a disease, what is happening in the UK as we move into autumn is lots of RT-PCR tests at a diagnostically meaningless cycle threshold are returning positive results from dead and non-infectious strands of virus from any of the family of coronaviruses, seasonal influenza, the common cold and other respiratory viruses, between which the RT-PCR test cannot distinguish.
- ‘One way to help you stay safe is to get a coronavirus vaccine. The coronavirus vaccine should stop you getting very poorly if you do catch coronavirus.’ In fact, as I showed in Part 1 of this article, far from COVID-19 ‘vaccines’ reducing the severity of symptoms of coronavirus disease, the data from PHE shows that a higher number and percentage of ‘vaccinated’ people are being admitted to emergency care in UK hospitals than those who haven’t been ‘vaccinated’.
- ‘There is a small chance that you can still catch coronavirus if you have had the vaccine.’ In fact, far from reducing the chances of being infected with SARS-CoV-2, the data from PHE shows that a higher number and percentage of ‘vaccinated’ people are returning a positive RT-PCR test.
- ‘After your vaccine your arm might be a bit sore for a short time. You might also feel tired or have a headache. This is called having side effects.’ In fact, as of 8 September, the ‘side effects’ reported to the MHRA following injection with the Pfizer/BioNTech ‘vaccine’ include: 10,916 blood disorders (of which 3 have been fatal); 5,339 cardiac disorders (95 fatal); 4,421 ear disorders; 5,340 eye disorders; 30,049 gastrointestinal disorders (16 fatal); 80,874 general disorders (183 fatal); 1,634 disorders of the immune system (2 fatal); 7,545 infections (84 fatal); 4,843 injuries (1 fatal); 1,786 metabolic disorders (1 fatal); 38,603 muscle and tissue disorders; 218 neoplasms (4 fatal); 55,949 disorders of the nervous system (53 fatal); 6,611 psychiatric disorders (1 fatal); 867 renal and urinary disorders (7 fatal); 18,710 reproductive and breast disorders (1 fatal); 13,797 respiratory disorders (49 fatal); 22,425 skin disorders (1 fatal); and 5,148 vascular disorders (13 fatal). This huge and disproportionate number of adverse drug reactions, which itself represents between 10 per cent and 2 per cent of estimated ADRS, is completely inadequately represented by the consent form’s dismissive reference to a sore arm, tiredness or a headache. Above all, it fails to make any mention of the greatly increased risk of myocarditis and pericarditis in children and young adults following injection with ‘vaccines’ employing the experimental mRNA biotechnology used by Pfizer.
- ‘You don’t have to do keep following the governments rules if you have been vaccinated but they will help you to stay safe. This includes social distancing, wearing a face covering and washing your hands carefully and often.’ In fact, there is not, and never has been, any medical justification for either social distancing or wearing a face covering, which have been imposed purely in order to create the illusion of a health emergency and encourage compliance with the biosecurity measures they have helped to justify. More importantly, this statement, the final one in the form and the one most designed to influence children, quite clearly contains an extra-medical inducement to be injected, and is therefore in violation of the principles and laws of voluntary consent without coercion or ulterior inducement.
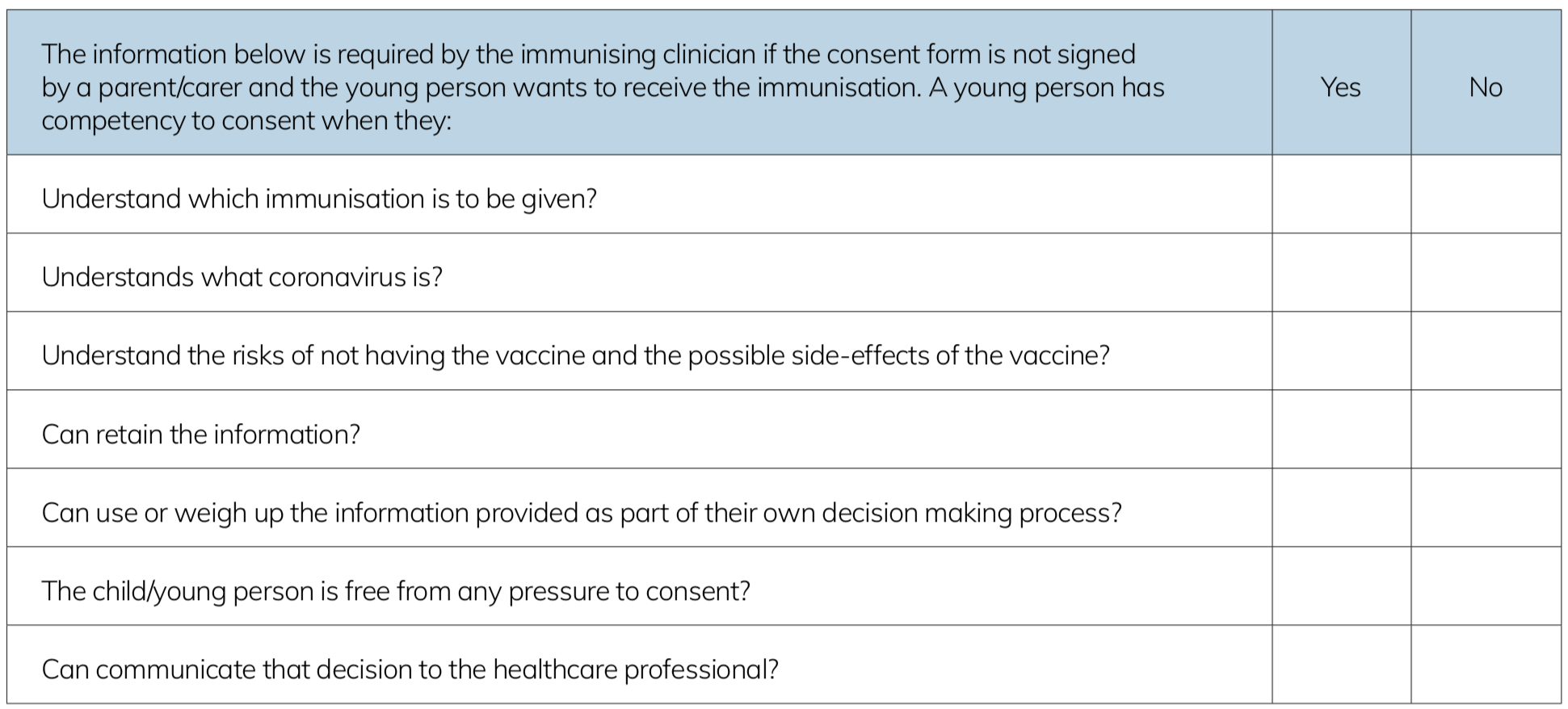
The final part of the form contains a ‘Gillick guidelines checklist’ (above) for the clinician who is injecting the COVID-19 ‘vaccine’ into the child. I challenge any clinician to show how a 12-15-year-old child, on the basis of the inaccurate and inadequate information contained in this consent form, let alone in the conditions in which the programme has been implemented, can possibly understand what immunity will be conferred by the ‘vaccine’, what coronavirus is and the threat it presents to them and others, the risk of having and not having the ‘vaccine’, retain information that has not been supplied for them, weigh up the inaccurate, inadequate and misleading information they have been given to making their own decision, and be regarded as free from pressure and coercion to consent. And I remind them that, in the best practice guidelines on consent outlined in the Green Book, it states:
‘It is a legal and ethical principle that valid consent must be obtained before starting personal care, treatment or investigations. Healthcare professionals (or other non-registered healthcare workers) who do not respect these principles may be liable to legal action and/or action by their professional body.’
So how did we get to this point, where the UK biosecurity state, on the guidance of unelected technocrats in a revolving door between the pharmaceutical companies that fund them and advisory posts to the UK Government that defers to them, is about to subject 3.15 million British children to injection with experimental, temporarily authorised ‘vaccines’ that neither immunise them against SARS-CoV-2 nor stop its transmission, on the justification of protecting them from a disease to which they are statistically immune? How did this criminal, sinister and obscene programme become — if not yet a condition — then already an example of civic virtue in the UK biosecurity state?
3. Virtue and Terror
On 23 July, 2021, the Scottish actor and former bodybuilder, Michael Mitchell, who had appeared in the films Braveheart and Gladiator and won numerous Fitness World Championships, died at the age of 65 while on vacation in south-west Turkey. Police are conducting an investigation, but the press concluded that a heart attack was the probable cause of death. Five months before, on 22 February, Mr. Mitchell had announced on his Twitter account that he had been injected with his first dose of CoronaVac, a COVID-19 ‘vaccine’ developed and manufactured by the Chinese pharmaceutical company, Sinovac Biotech Ltd, and whose phase 3 clinical trials are being conducted in, among other countries, Turkey. Mr. Mitchell wrote: ‘Absolutely zero side effects. Looking forward to 2nd one’. This arrived the following month, on 20 March, when he again announced: ‘Zero after effect (as yet). Vaccine certificate issued’. On 2 May, Mr. Mitchell posted a photo of himself smiling, circled by a banner declaring himself to be ‘fully vaccinated’. As if to reassure himself, on 6 May he posted a statement that, of 150 million ‘vaccines’ administered, only ‘0.005% may have resulted in a serious side effect’. Two months later, on 16 July, Mr. Mitchell announced: ‘Well, that’s my third jab today. Proud to be part of this experiment to save lives’. He later confirmed that this ‘booster’ dose was the Pfizer manufactured ‘vaccine’ developed by BioNTech. On 21 July, Mr. Mitchell posted a long statement about his choice to go on wearing a face covering beyond the legal requirements in Turkey. These included contributing to the ‘common good’, wanting to be ‘part of the solution, not the problem’, feeling like ‘an adult contributing to the security in our society and I want to teach others to do the same’, being ‘caring and responsible’, and advocating that ‘if we could all live with the consideration of others in mind, the whole world would be a much better place’.
Now, none of these reasons are contemptible, and some of them I share, although his fears about security in our society reveals collective anxieties the coronavirus crisis has elevated to a global neurosis. I quote them here, therefore, not to ridicule Michael Mitchell, who two days later was dead, but as an example of the employment of both virtue and terror in the global COVID-19 ‘vaccination’ programme. For Mr. Mitchell, getting ‘vaccinated’ was an act of virtue, which he was keen to advertise and promote, even to the point of describing his taking multiple doses of different ‘vaccines’ as an experiment ‘so we may learn more about a way forward’. However, for those who do not display the same virtues, there is the increasingly realised threat of being ostracised from society, of discrimination, of fines for non-compliance, of enforced isolation and, eventually, of imprisonment. I do not know what killed this extremely fit 65 year-old 2 days after he was injected with a drug by one of the most litigated and corrupt pharmaceutical companies in the world, whose vast profits alone have allowed it to escape prosecution for malpractice and manslaughter; but in this section I want to look at how the UK ‘vaccination’ programme has been pushed on the British public through this combination of the revolutionary principles of virtue and terror.
Following the foundation of the First French Republic, the Reign of Terror (in French ‘la Terreur’), which ran roughly from the establishment of the Revolutionary Tribunal in March 1793 to the death of Maximilien Robespierre the following July, was overseen by the Committee of Public Safety (Comité de salut public). Initially, at least, this might seem like a strange name for a revolutionary organisation whose administrative and executive powers over the armed forces, the judiciary and the legislature empowered it to launch a campaign of persecutions, denunciations, arrests, imprisonments without trial and public executions that killed maybe 27,000 French citizens under the flag of ‘virtue’. But for Robespierre, under whose leadership the Committee of Public Safety became the de facto war-time government of France, the safety of the French Republic depended on the virtue of each and every French citizen, and anyone who failed to display such virtues must be forcibly removed from the body politic. In his famous speech to the National Convention on 5 February 1794, On the Principles of Political Morality, Robespierre clarified the symbiotic relationship between virtue and terror:
‘If the mainspring of popular government in peacetime is virtue, the mainspring of popular government during a revolution is both virtue and terror; virtue, without which terror is fatal; terror, without which virtue is powerless. Terror is nothing but swift, severe, inflexible justice; it is therefore an emanation of virtue. It is less a principle in itself than a consequence of the general principle of democracy, applied to our nation’s most pressing needs.’
In Part 1 of an article I published last year, The New Normal: What is the UK Biosecurity State?, I sought to situate the programmes and regulations of the UK biosecurity state within the political and juridical history of ‘states of emergency’. My guide in this — as in so much about the revolution we’re witnessing of formerly liberal democracies into biosecurity states — was the writings of the Italian philosopher, Giorgio Agamben, who in his book, State of Exception, traces this history back to the French Revolution. By the time Robespierre made this distinction between the virtue of peacetime government and the terror of revolutionary government, the former National Constituent Assembly had itself distinguished, in the decree of 8 July, 1791, between a state of peace (état de paix), in which civil and military authorities act in their own separate spheres, a state of war (état de guerre), in which civil authority must act in concert with military authority, and a state of siege (état de siège), in which the functions of civil authority in maintaining order and policing passes to the military commander. But this distinction didn’t long survive. Agamben writes:
‘The subsequent history of the state of siege is the history of its gradual emancipation from the wartime situation to which it was originally bound in order to be used as an extraordinary police measure to cope with internal sedition and disorder, thus changing from a real, or military, state of siege to a fictitious, or political one.’
On 26 March, 2020, the day after Parliament voted itself into recess, the Secretary of State for Health and Social Care, Matt Hancock, unlawfully exercising powers conferred by Section 45c of the Public Health (Control of Disease) Act 1984, made the Health Protection (Coronavirus, Restrictions) (England) Regulations 2020 into law. Regulation 3, ‘The emergency period and review of need for restrictions’ — although superseded by later regulations — made it clear that, without it being formally declared by the UK Government, the UK was now in a de facto state of emergency. Unlike the emergency powers conferred by the Civil Contingencies Act 2004, which must be reviewed by Parliament every 30 days, this ‘emergency period’, during which many of our fundamental human rights and civil liberties have been removed indefinitely, can itself be extended indefinitely by the UK Government. Made without a draft having been laid before or approved by both Houses of Parliament, and without evidence of their proportionality or an assessment of their impact, these Regulations initiated an emergency period that will only end at a time specified by the Secretary of State.
It is under this fictitious — which is to say, politically-declared — emergency period that, a year later, the powers conveyed by the Coronavirus Act 2020 were extended for the second time by a vote of 484 MPs to 76 up to September 2021; and, as of writing, 501 coronavirus-justified Statutory Instruments have been made into UK law by decree of the relevant Minister. Most crucially, for the purpose of this article, it is on the justification of this fictitious emergency period that the various brands of COVID-19 ‘vaccines’ have been temporarily authorised in the UK by the Medicines and Healthcare products Regulatory Agency before they have completed their trials, and their developers, manufacturers, advertisers, administers and other agents all indemnified against the consequences of their use. Unless there is a hugely increased level of rebellion among Conservative MPs or actual opposition from Labour MPs, on some still undeclared day over the next fortnight, the Coronavirus Act will be extended for the third time for a further 6 months to 24 March, 2022, allowing the Government to continue and extend the UK ‘vaccination’ programme to children under the age of 16. According to the Government’s COVID-19 Response: Autumn and Winter Plan, which it published this month, some of the Act’s powers will be repealed, including the notorious Schedule 21, ‘Powers relating to potentially infectious persons’, and Schedule 22, ‘Powers to issue directions relating to events, gatherings and premises’. However, the Government is extending The Health Protection (Coronavirus, Restrictions) (England) (No. 3) Regulations 2020, which empowers the Secretary of State to direct local authorities to close or restrict or impose requirements on entry to private premises, events, public outdoor places, and to enforce such powers, issue fixed penalty notices for non-compliance, and prosecute those who fail to comply. The Plan explicitly states that the legal basis for imposing these restrictions on our human rights and civil liberties in England is The Public Health (Control of Disease) Act 1984, and that ‘no changes to The Public Health Act are planned’. Legislatively and legally, then, we are still living under emergency powers.
Just as for the French people during the Terror, the civil liberties and human rights of the British people during this ongoing emergency period are being determined by our own Committee of Public Safety, with whose name we are all familiar by now. The Government-appointed, pharmaceutical-industry funded members of the Scientific Advisory Group for Emergencies (SAGE) decide on a range of medically unjustified biosecurity restrictions, from the imposition of lockdowns to the injection of our children with experimental ‘vaccines’, all of which have demonstrably and repeatedly failed to do anything to stop the spread or impact of this seasonal respiratory virus. On the contrary, the ultimate function of the restrictions and programmes justified by SAGE — from social distancing, compulsory face coverings, RT-PCR tests and digital tracing apps to closed businesses and public spaces — has been the creation and maintaining of the public’s faith in the existence of this public-health emergency.
Under this politically-declared state of emergency, in which the legislature has largely and repeatedly been bypassed by the executive in order to exert and expand dictatorial powers over the electorate, the UK public, as in Revolutionary France, is required at all times to demonstrate commitment to, and demonstration of, the virtues of biosecurity. As I have argued previously, most fully in Cui Bono? The COVID-19 ‘Conspiracy’, these are properly revolutionary values, implementing the public’s ideological conversion to, and support for, the New World Order of global biosecurity under a nationalised system of totalitarian population control, the next stage of which is the mandating of ‘vaccine’ passports. And just as they had under the Committee of Public Safety, those values have their basis in both virtue and terror.
Of course, I’m not suggesting for a moment that the Conservative Government of Boris Johnson shares, even in principle, the virtues of the First French Republic. The UK biosecurity state has not emerged from a bourgeois revolution against nearly 950 years of absolute monarchy but from 40 years of neoliberalism, and the new form of governance is above all a takeover of civic authority and parliamentary democracy by global corporate power in its crudest form, which is in no way limited to the pharmaceutical industry. But that doesn’t mean that the leaders of our formerly liberal democracies — among whom is the great burlesque dancer of our day, who has always treated British politics as the stage for his personal rake’s progress — aren’t above covering their bloody maws with the medical mask of civic virtue.
We are all familiar, by now, with that defining political gesture of our era, ‘virtue signalling’, which even those largely convinced of the necessity of — or at least the lack of danger in — wearing face-coverings and getting injected with experimental drugs have used to describe the public displays of moral superiority by the masked and ‘vaccinated’. But if we take this contemporary phrase precisely, as it was imposed by the Committee of Public Safety under Robespierre, we can already see that what started as ‘virtue signalling’ in public and on social media is in the process of becoming a requirement not just of civic duty but of legal compliance and, through ‘vaccine’ passports, of our status as a citizen. And we know — too well already — the other side of this coin, which is the apparently unlimited violence the virtuous are ready to see inflicted on those who refuse to comply with the cultic practices of virtue.
The fact that French citizens who, under the reign of the Terror, failed to demonstrate the virtues of the new French Republic were thrown into prison or sentenced to death by the Revolutionary Tribunal doesn’t make the proposed demotion to second-class citizens prohibited from international travel, public life, medical care, education and gainful employment of those of us who fail to demonstrate the virtues of the UK biosecurity state any less a manifestation of the terror without which all this virtue-signalling is powerless. Indeed, the implementation of the ‘vaccination’ programme has exhibited, with all the force and familiarity of history, the co-existence of virtue and terror in implementing this Fourth Industrial Revolution. As an example of which, I want to look at some articles published in the popular press in which the terror behind the virtue of the COVID-faithful has raised the blade of its guillotine for all to see.
My first example is the columnist, Richard Littlejohn, writing in the Daily Mail on 18 February, 2021, two months after the first ‘vaccine’, Pfizer, was authorised for temporary use in the UK.
‘If some people don’t like the idea of getting the jab, tough. I wouldn’t force them. But maybe refuseniks should have to wear a bell round their necks and sport a sandwich board declaring themselves “Unclean”. If that means no jab, no job: No problem. It’s a no-brainer.’
The term ‘refusenik’ was used in the Soviet Union to describe Jews and other ethnic and religious minorities denied permission to emigrate to Israel and other diasporas, with the applicant being noted by the authorities and either fired from their place of employment or banned from their profession. The following month, on 19 March, an anonymous article in the Daily Mail repeated this description of people who refuse to be injected with the COVID-19 ‘vaccines’ as ‘refuseniks’. As is now the imposed norm in coverage of the coronavirus crisis in the media, rather than interviewing doctors, scientists, lawyers or political commentators, the article reported the comments of working people — including a housewife, a chef, a grocer, a builder and a salesman — whom it dismissed as ‘conspiracy theorists’. These interviews were accompanied with negative visual depictions of the ‘refuseniks’ (below left), which were contrasted with photographs of masked members of the public patiently queuing — that most English of virtues — to be injected at ‘vaccination’ centres.


Drawing, admittedly, on the discourse of racism exported across the globe by the slave trade of the British Empire, this equation between non-compliance with biosecurity state laws and biological degeneracy was pioneered by National Socialist eugenicists and propagandists for the enforced euthanasia and sterilisation programme, who depicted ‘subjects of the state’ that had been deprived of citizenship by the Reich Citizenship Law of 1935 as a biological danger not only to the Aryan race but also to the Third Reich. But before its current revival in the UK biosecurity state, we saw this equation between dissidence and degeneracy employed in the security campaign launched in November 2016 by the British Transport Police, which used ethnic stereotypes of Arabs and Asians to depict suspected terrorists threatening the white population of London (above right). It was only when comparisons were drawn between this fearmongering and the propaganda of the Third Reich that some of the posters were withdrawn from use (although the campaign continues, lost though it is amid the relentless fearmongering of biosecurity propaganda). Perhaps because they were made on the accusation of racism, these comparisons were for once deemed valid, rather than denounced — as they are when applied to the UK biosecurity state — as insults to the memory of the ‘Holocaust’ (etc). For there have been no such complaints made about the equivalent strategies used by the British Government and UK media to pathologise and stereotype those who enact their protected right, under UK law, to choose not to be injected with these still experimental and dangerous ‘vaccines’. Quite the contrary.
Although the UK Government would doubtless disown the Daily Mail articles, it’s the biosecurity state’s campaign of terror that has authorised the use of this language of incitement by the UK media. And as the terror increases, it’s use hasn’t been restricted to the tabloids, but has been eagerly and even fervently adopted by the broadsheets, whose comfortably liberal and politically-correct columnists have joined the pogrom like so many virgins at an orgy. On 27 February, the columnist Nick Cohen, in an article in the Guardian provocatively titled ‘It’s only a matter of time before we turn on the unvaccinated’, wrote:
‘Rational people will ask why they should continue to accept restrictions on their freedoms because of ignorant delusions. Employers will demand to know what possible argument there is against allowing the owners of pubs, airlines, restaurants, hotels or holiday homes to demand proof of protection when immunity passports might save their business. To make it personal, how would you feel come the autumn if someone you love contracted cancer and the NHS delayed treatment because it had to look after needlessly ill Covid patients? . . . How long this relaxed state will last as demands to punish the unvaccinated grow is another matter.’
On 23 March, Sean O’Grady, the associate editor of the Independent, came up with this justification for violating the Nuremburg Code, the European Convention on Human Rights, the Universal Declaration on Bioethics and Human Rights, and National Health Service best practice, that medical intervention must not be subject to coercion, in particular targeting the right to education of UK children under the United Nations Convention on the Rights of the Child:
‘We do not permit certain doctors from practicing if they refuse to take a jab for hepatitis, and the principle is the same. It is lawful and fair discrimination — and if people don’t want a jab, they can work elsewhere. They have no human right to any given job, as some pretend. This is an absurd proposition. Indeed, I would go even further: if trials proved they were safe, I would vaccinate every child old enough to receive it, as a condition of receiving a state education.’
Two months later, on 17 May, Shelagh Fogarty, to whom I once gave an interview about the legacy of the Grenfell Tower fire, during which she reacted as a concerned liberal, nonetheless didn’t hesitate to say live on LBC Radio:
‘I’d literally be in fights with these people (vaccine decliners). How do you keep seeing them at work without wanting to poison their coffee?’
The following day, Sarah Vine, the former arts editor for The Times, revived the ‘refusenik’ accusation in her column in the Daily Mail, to which she added the suggestion that refusing a COVID-19 ‘vaccine’ was at best a criminal act, at worst an act of terrorism:
‘We can’t let idiots who don’t want Covid vaccines hold us hostage. You are stupid. Weapons grade stupid. So I’m totally on the side of Lord (Andrew) Lloyd-Webber when he says refusing the jab is no better than drink-driving. It’s an act of supreme selfishness and irresponsibility. Not least because it won’t be the vaccine refuseniks who are left to clear up the mess, but the NHS.’
Not to be outdone, that same day Sean O’Grady, in another article in the Independent titled ‘This is what we do about anti-vaxxers’, outlined a programme that wouldn’t have looked out of place among the various ‘laws for the protection of the people’ in 1930s Germany:
‘No jab, no job; no jab, no access to NHS healthcare; no jab, no state education for your kids. No jab, no access to pubs, restaurants, theatres, cinemas, stadiums. No jab; no entry to the UK, and much else. As I say, with rare exceptions of genuine medical justification, everyone who refuses a vaccine could be a killer on the loose, and should be judged accordingly.’
I hope one day that history, and a law court, will judge Mr. O’Grady for these words. In the meantime, in July The Times used the term ‘refusenik’ to describe university students who have not been injected with a COVID-19 ‘vaccine’; with the Daily Record reporting the Conservative MP, Michael Gove, saying that such ‘refuseniks’ were ‘selfish’ and should be banned from mass events. While earlier this month, the Financial Times used the term to describe the millions of European citizens enacting their right to protest against the imposition of the Green Pass ‘vaccine’ passport in France and Italy. These, remember, are the same newspapers that reacted with horror when an anti-lockdown demonstrator, Kate Shemirani, perhaps ill-advisedly promised a second Nuremberg Trial for the clinicians administering the UK ‘vaccination’ programme that has already claimed so many lives; and who denounced as ‘inciting hatred’ any suggestion that the CEOs, scientists and politicians complicit in the development, manufacture and authorisation of the COVID-19 ‘vaccines’ should be held to account.
There has been, and there will be, a lot more and a lot worse of this emanation of terror from virtue, as the public is emboldened by this campaign of fear, hate, disgust, dehumanisation and advocacy of open apartheid against the non-compliant. ‘Refusenik’ is only the latest term of denigration, and it won’t be the last. ‘COVID-denier’, ‘covidiot’, ‘vaccine hesitant’, ‘anti-mask’, ‘anti-science’, ‘conspiracy theorist’ — these are the accusations of the COVID-faithful in this global staging of the Salem Witch Trials, in which COVID-19 is the devil seen everywhere by every coward hoping to save his own skin, every signaller of biosecurity virtue, every petty advocate of state terror. As the UK ‘vaccination’ programme enters its final stage, ‘murderer’ is the accusation being used online with increasing frequency and greater confidence to describe those who refuse to comply. And it’s on this media campaign of hate, scapegoating, public denunciation and calls for violent retribution that the Government has justified the more than 500 coronavirus-justified statutory regulations made into law in the past 18 months — at an extraordinary rate of nearly 1 per day. Yet in their public display of obedience to the dictates of COVID-compliance, what none of these propagandists of terror has dared to question is the new form of unelected and unaccountable corporate governance these regulations have been used to construct in front of our eyes and without opposition from the putative defenders of liberal democracy. But then, they know the iron blade of terror waiting behind the velvet cloak of virtue, and that the full power of the UK biosecurity state is suspended over their heads as much as ours. At the conclusion of his speech to the National Convention, Robespierre declared:
‘We must smother the internal and external enemies of the Republic, or perish with it; and in this situation, the first maxim of our policy should be to lead the people by reason, and the enemies of the people by terror.’
4. Crime and Punishment in the UK Biosecurity State
On 16 January, 2021, Dr. Stephen Wright, a healthy 32-year-old child psychologist and married father of two children, updated his Facebook profile picture. A photograph of himself and his wife, Charlotte, taken at their wedding in June 2018, now bore the NHS logo and a white circle in which a crown and heart were surrounded by the declaration: ‘I’ve had my COVID vaccination’. It was later revealed to be the AstraZeneca ‘vaccine’. Dr. Wright had just been promoted to his new position as Senior Clinical Psychologist at Great Ormond Street Hospital in London, and was due to start on 1 February.
Instead, in the early hours of 26 January, 10 days after his injection, Dr. Wright suffered what was later diagnosed as a cerebral venous stroke. The previous evening he had fallen asleep after refusing dinner, and when he awoke complained of pins and needles. With his arm moving uncontrollably, his wife called an ambulance and by the time the paramedics arrived Dr. Wright’s blood pressure was so high they advised him to visit hospital for further checks. Due to coronavirus-justified regulations, his wife was not permitted to accompany him to King’s College Hospital. Two MRI scans revealed massive bleeding on the brain, and he was placed on life support. Later that day he died. At his request, Dr. Wright’s organs were donated, and his wife reported that his lungs went to a man in his thirties and his heart to a teenage boy. His wife subsequently told The Independent that she ‘does not disagree with the rollout’ of the COVID-19 ‘vaccination programme’; adding: ‘I know why they had to do it and that they had to do it.’
It is a characteristic of the new form of corporate governance under which we are now living — in which our rights and freedoms are no longer determined by laws made by our elected representatives in Parliament and adjudicated by courts of law, but instead decided by unelected and largely unknown technocrats — that not only the political but also the financial, juridical, security, military, medical, media, educational and cultural institutions of the nation have all collaborated in effecting the compliance of the population — willingly or otherwise — with the revolutionary virtues of the New Normal. To measure just how far virtue has brought us on the road to terror — and to remind ourselves how swiftly, severely and inflexibly what yesterday were dismissed as ‘conspiracy theories’ have become today’s revolutionary justice — we could do worse than read the House of Commons briefing paper, dated 27 July, 2021, titled ‘Coronavirus: enforcing restrictions’. In this section I’m going to summarise its findings.
The briefing begins by specifying the range of organisations and individuals that are responsible for enforcing what it calls ‘coronavirus restrictions’, demonstrating that the UK biosecurity state is forming a totalitarian society in which distinctions between public and private will no longer exist and everyone will be compelled, at all times and in all places, to subject themselves and others to a constant surveillance, monitoring and control. These restrictions are divided in the briefing into 1) lockdown, 2) face coverings, 3) international travel quarantine and 4) self-isolation.
1) To enforce lockdown restrictions, police officers and police and community support officers (PCSOs) have formal powers to enforce regulations. Local authorities, in the form of Environmental Health Officers and Trading Standards Officers, have the power to enforce restrictions on businesses, and to prosecute those which fail to comply. In addition, to encourage compliance, the Government has provided local authorities with £30 million of funding for the deployment of coronavirus marshals to report on those who have failed to comply.
2) To enforce face coverings, police officers and PCSOs have formal powers to enforce the requirement in relevant places. Transport workers can deny travel to those not complying, and Transport for London enforcement officers have additional powers to issue Fixed Penalty Notices (FPNs). However, business owners are also obliged to display signs reminding customers of their obligations to wear a face covering; and under health and safety legislation, liability law and the law on negligence, they are obliged to ensure that their business is ‘COVID secure’.
3) To enforce international travel quarantine, commercial transport services are obliged to ensure that passengers have a negative test result for SARS-CoV-2 no more than 72 hours before departure. The Civil Aviation Authority has the power to issue Fixed Penalty Notices to commercial transport services who do not meet their coronavirus obligations. Border Force officials conduct ‘biosecurity checks’ on every person arriving in the UK, and have powers to issue FPNs to passengers. According to the briefing, the Government claims that Public Health England’s Isolation Assurance Service (IAS) makes 3,000 calls every day — successfully contacting 1,500 people — to check they are complying with international travel quarantine restrictions and to collect information on their health status. NHS Test and Trace carry out up to 1,000 visits a day to ensure those required to quarantine are doing so. Staff have no powers of enforcement, but can contact police and PCSOs should they have concerns about compliance. On 27 January, 2021, the Home Secretary said that police had ‘stepped up checks and are carrying out more physical checks at addresses to ensure that people are complying with the rules’.
4) To enforce self-isolation, UK citizens are legally required to self-isolate when NHS Test and Trace informs them that they, or someone they have been in contact with, has tested positive for SARS-CoV-2. The public may report potential breaches of self-isolation directly to the police. When they receive report of a suspected self-isolation rule break, the police should contact NHS Test and Trace, which will then share the following information with the police:
-
- first and last name of the individual;
- home address and telephone number;
- period of self-isolation;
- date notification to self-isolate was received;
- details of how the individual was notified by Test and Trace, including address, telephone number and email address where relevant;
- date of birth;
- whether the individual has a positive RT-PCR test or is a close contact of someone who has;
- a copy of the notification issued by Test and Trace;
The police will conduct a risk assessment of the report and, if they regard it as appropriate, visit the address provided by the individual to determine compliance. But, in addition, employers are required not to knowingly allow their workers to break their self-isolation, and those who fail to meet this requirement commit a criminal offence.
The result of this collaboration between public organisations and private businesses to create a totalitarian society that is still in formation is that, in the 15 months between 27 March, 2020 and 20 June, 2021, 117,213 Fixed Penalty Notices (FPNs) have been issued in England and Wales under lockdown regulations (below). And while, during the first national lockdown, between 27 March and 1 June, 2020, police issued an average of 1,553 FPNs per week, during the third national lockdown, between 6 January and up to 17 March 2021, this number tripled to an average of 4,491 FPNs per week. Contrary to media representation, therefore, of an easing off of the restrictions under which we are living, the punishments for disobedience are increasing significantly in both number and severity. In addition, 3,767 FPNs have been issued under regulations on face coverings, 737 FPNs under regulations on international travel, and, up to 16 May, 187 FPNS under regulations on self-isolation.
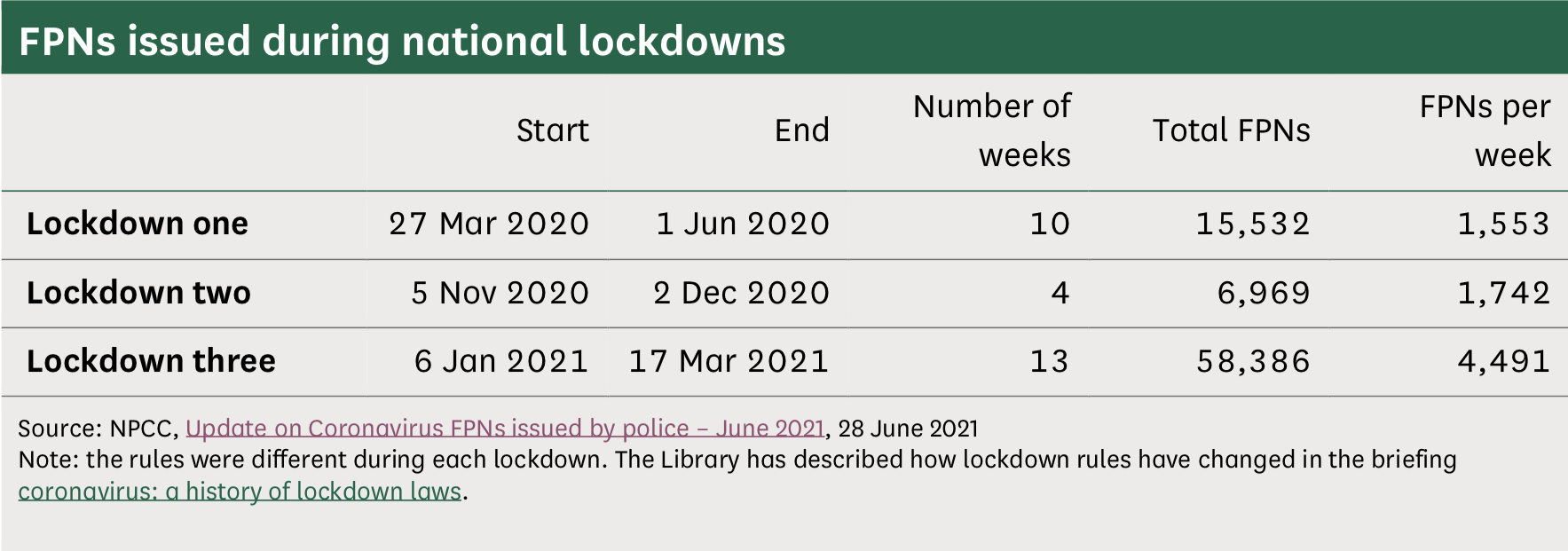
To accommodate this mass criminalisation of the UK public without creating an equally vast backlog of court cases, Fixed Penalty Notices enact what the briefing calls ‘a form of out-of-court criminal outcome’. These offer the accused who can afford to the chance to avoid criminal proceedings by paying the fine within 28 days, while creating sufficient incentive in those unable to afford the fine to avoid offending against the vast numbers of new laws.
However, as the former Justice of the Supreme Court, Lord Sumption explained in his lecture on ‘Government by Decree: COVID-19 and the Constitution’, which he delivered to the Cambridge Private Law Centre last October, while FPNs have been in use since the early 2000s, they are normally authorised in modest amounts for minor regulatory infractions such as parking and the lesser driving offences. In contrast, the nearly 500 coronavirus-justified statutory regulations made into law during the ongoing ‘emergency period’ politically declared by the UK Government has authorised the use of FPNs for a vastly increased number and variety of newly created offences, for increasingly large fines, and far in excess of any fine that would be impose by a law court for such an offence.
In confirmation of this vast expansion in the use and severity of Fixed Penalty Notices as both a deterrent to, and a punishment for, failing to comply with the thousands of restrictions implementing and maintaining the UK biosecurity state, the briefing lays out the fines in tables (below). Since publishing this briefing in July, national lockdown has officially been lifted, and the wearing of face coverings is now Government guidance rather than mandated by regulations; and for this reason the FPNs for non-compliance with the relevant regulations have been removed from the briefing. However, the recent threat by the Secretary of State for Health and Social Care to reimpose both this winter, as rising cases of seasonal influenza continue to be misdiagnosed as SARS-CoV-2, indicates that we have not seen the last of either lockdowns or mandatory face coverings in the UK. Nor do I believe the record of the extraordinary fines imposed for non-compliance should be wiped from the record, as it has been from the revised version of the original briefing, as if they were never inflicted on the public in such vast numbers. And, fortunately, I made screen-grabs of the tables in the briefing before they were removed, which I reproduce here.
1) For not complying with lockdown restrictions under The Health Protection (Coronavirus, Restrictions) (Steps) (England) Regulations 2021, which were revoked on 18 July, the Fixed Penalty Notices were as follows:
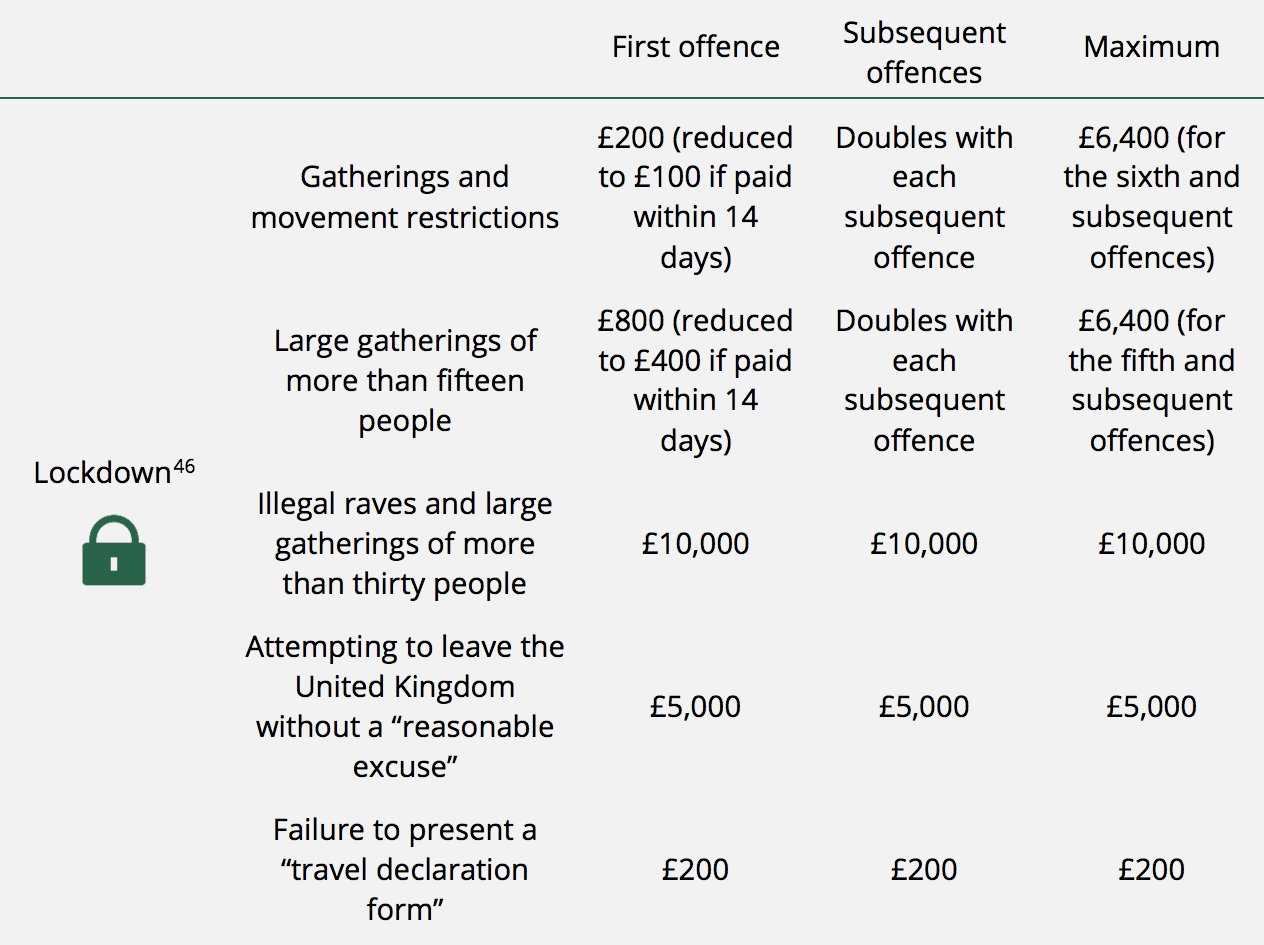
2) For not complying with face coverings where mandated under The Health Protection (Coronavirus, Wearing of Face Coverings in a Relevant Place) (England) Regulations 2020, and The Health Protection (Coronavirus, Wearing of Face Coverings on Public Transport) (England) Regulations 2020, both of which were also revoked on 18 July, the Fixed Penalty Notices were as follows:

3) Since they remain in effect under the Government’s COVID-19 Response: Autumn and Winter Plan, the Fixed Penalty Notices for not complying with international travel quarantine under The Health Protection (Coronavirus, International Travel) (England) Regulations 2020 remain in place, and have, indeed, been extended by The Health Protection (Coronavirus, International Travel and Operator Liability) (England) Regulations 2021, and are printed as follows in the updated briefing:
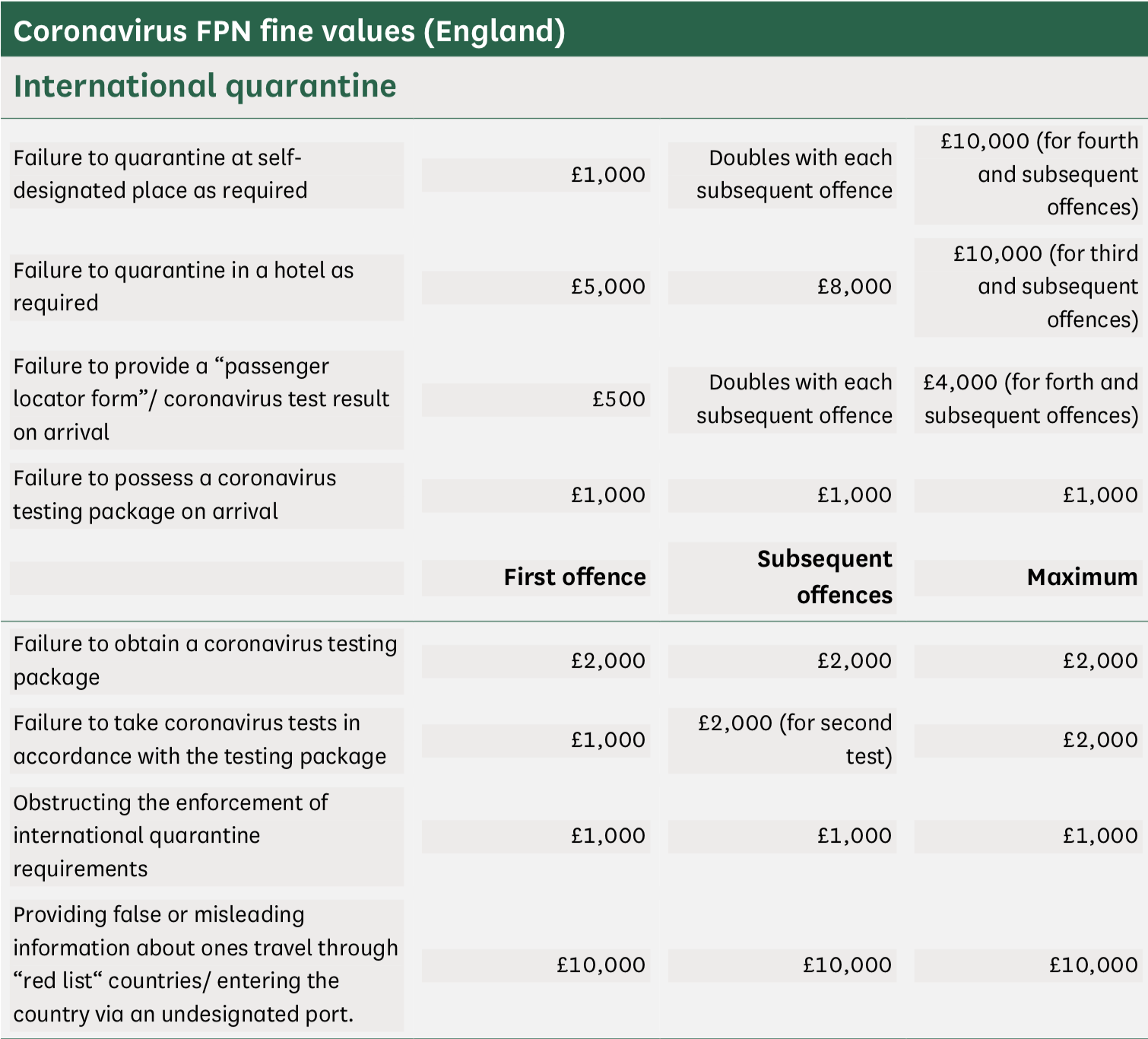
4) As do the Fixed Penalty Notices for not remaining in self-isolation under The Health Protection (Coronavirus, Restrictions) (Self-Isolation) (England) Regulations 2020, which are as follows:

The National Police Chiefs’ Council has reported that, in the 15 months between 27 March 2020 and 20 June 2021, they issued 366 Fixed Penalty Notices for large gatherings incurring a £10,000 fine. These included, but were not limited to, unlicensed music events, private parties and protests. As of 22 September, 2020, a year ago, 9,428 FPNs had been paid and 9,413 had not been paid. Those who do not pay may face criminal proceedings. In addition, 3,440 FPNs in England and 501 in Wales have been issued for a gathering of more than 15 people, incurring a fine of £800. In addition, those who provide false or misleading information to avoid hotel quarantine can be investigated for fraud, and those found guilty of the relevant fraud offence can be imprisoned for up to 10 years if convicted at a Crown Court. If convicted by a Magistrate, the sentence is a maximum of 12 months.
In the face of this vast web of newly-created regulations, offences and punishments, it’s useful to clarify what the police can and cannot do to enforce them, and anyone committed to resisting their unlawful enforcement should learn and remember by heart what the instruments of terror can do within the law. What they can and will do outside the law is already a matter of historical record and common experience.
Police can issue directions to individuals they suspect are breaching coronavirus-justified restrictions on gatherings, requiring them to disperse and return home. They can also issue ‘prohibition notices’ to businesses failing to comply with restrictions or requirements on businesses. Police officers can use ‘reasonable force if necessary’ to enforce coronavirus-justified restrictions. Police officers in England and Wales have an expanded power of arrest, which allows them to arrest those they suspect of lockdown offences for public order reasons.
However, although police officers have powers to enter private property in limited circumstances, they cannot use them to enter private property without consent to enforce lockdown regulations. And it is unlikely they would be able to establish whether a rule is being broken, and enforce it, if it has been. In contrast, Welsh police officers can enter someone’s home without permission when they have ‘reasonable grounds’ to suspect someone is breaking a lockdown law and consider it necessary, although it isn’t stated what those might be, or how they might be established when they can’t be in England. Officers in Wales can use reasonable force to enter private property in these circumstances.
The police conduct what the College of Policing calls ‘stop-and-account’, in which officers stop a member of the public and ask them what they are doing. However, there is no corresponding power to detain a person in order to talk to them or to ask them to account for themselves, and coronavirus-justified restrictions regulations do not — and never have — provided for one. Although we regularly are — and violently by armed and armoured gangs of the Metropolitan Police Service operating with impunity outside the law — a person cannot legally be arrested for not stopping to talk to an officer or answering their questions. Legally, members of the public are under no obligation to answer an officer’s questions during a stop-and-account, and can remain silent if they wish to do so.
The consequences of this already yawning and widening gap between even the vast array of new regulations made into law under the cloak of this manufactured crisis and the actions of an increasingly violent, armed and unaccountable police force are apparent to anyone who attended the anti-lockdown demonstrations this spring, or who has been fined or arrested for the new crimes of holding a party, sitting on a park bench, not wearing a mask or attending a protest. And the institutional racism of the UK police has been given as free reign here as it is when enforcing all the other restrictions on our rights and freedoms. Statistics show that Black, Asian and Minority Ethnic people were 1.6 times more likely to be issued a Fixed Penalty Notice than White people. Despite making up only 14 per cent of the resident population, young men aged between 18 and 24 across all ethnic groups accounted for an extraordinary 57 per cent of those issued FPNs. And young Black, Asian and Minority Ethnic men aged between 18 and 34 were twice as likely to be issued an FPN as their White peers.
In every respect, then, the guidance and regulations of the UK biosecurity state has authorised and exaggerated the racism, violence and unaccountability UK police forces. Indeed, the campaign of terror authorised by the executive of this constitutional dictatorship has been such that the police have gone far beyond the limits of these vastly increased and expanded laws in enforcing compliance on a terrorised and bullied population. Of the 1,631 people in England and Wales charged with a coronavirus regulation offence between 1 May 2020, and 30 June 2021, 319 were incorrectly charged, an error rate of 21 per cent (below). But then, as Robespierre argued, virtue without terror is powerless, and no abuse of power will not be excused in educating the public in its new civic duties of obedience, compliance and collaboration with the UK biosecurity state.
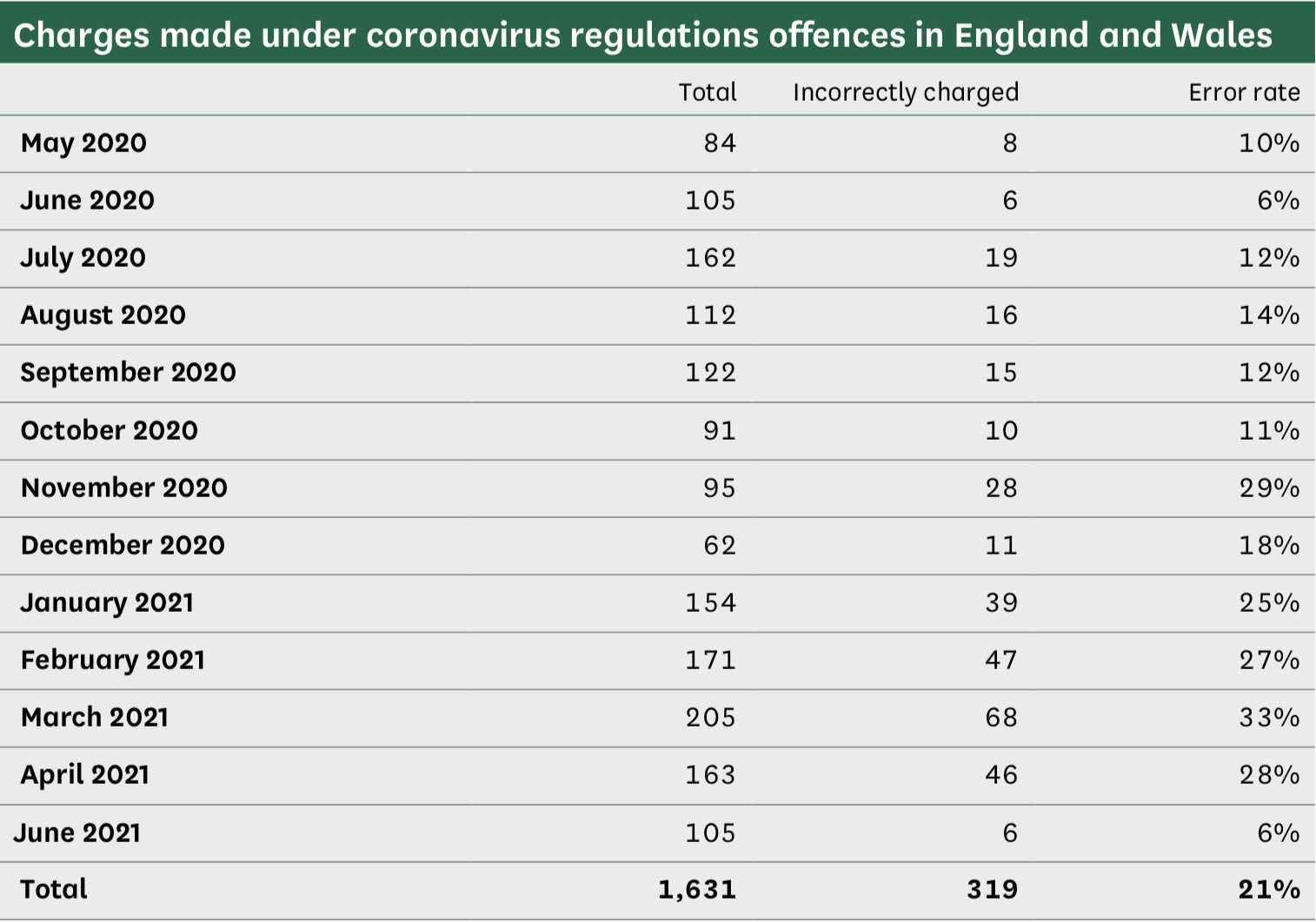
As we’ve already seen, the severity with which the regulations of this totalitarian society in formation are being imposed, and failure to comply punished, is increasing, not lessening; and the briefing attributes this to a unified political decision to police the UK public with greater severity. At the start of the third national lockdown, Cressida Dick, Commissioner of the Metropolitan Police Service, said rule breakers are ‘increasingly likely to be fined’; while Martin James Hewitt, Chairman of the National Police Chiefs’ Council, echoed the journalists we looked at above in equating refusal to comply with a lack of civic virtue, rather than a political and moral choice to resist these dictatorial and intrusive decrees:
‘After ten months of dealing with the situation, and with varying national regulations and measures firmly in place again across the UK, everyone should now understand the rules in their area. We all know for example that large gatherings should not be happening. Forces will continue to bear down on that very small minority who flagrantly and selfishly breach the regulations, such as those that organise unlicensed music events or parties. This behaviour puts others at significant risk and it’s right that we patrol in potential hotspots and that officers are inquisitive when they see something out of the ordinary. This will offer both reassurance to the public and act as a deterrent to those who think the measures don’t apply to them.’
In support of this declaration of the right of the police to assume the roles of spy, inquisitor and judge, the College of Policing, in its guidance on policing the third lockdown regulations in England, issued new advice to enforce ‘without repeated attempts to encourage people to comply with the law’ when people ‘do not respond appropriately’. Finally, Priti Patel, the most authoritarian, corrupt, unaccountable, violent and immoral Home Secretary in my lifetime, and the Minister responsible for turning what were made into law as temporary emergency powers to respond to an external threat to public health into a permanent state of emergency authorising new and expanded police powers to crush internal political dissent and social disorder, declared:
‘The vast majority of the public have supported this huge national effort and followed the rules. But the tragic number of new cases and deaths this week shows there is still a need for strong enforcement where people are clearly breaking these rules to ensure we safeguard our country’s recovery from this deadly virus. Enforcing these rules saves lives. It is as simple as that. Officers will continue to engage with the public across the country and will not hesitate to take action when necessary.’
Unfortunately, it’s very far from being as simple as the Home Secretary affects to believe, and not merely because it has been repeatedly shown that these ‘rules’ have done, and continue to do, nothing to ‘save lives’, as she claims, but have, on the contrary, killed tens of thousands of UK citizens. But they are very far from being the useless and harmful ‘measures’ of an incompetent Government.
In the same month this House of Commons briefing paper was published, the Government announced a £1 billion New Prisons Programme to build 4 new prisons for adult males across the UK, the first of which will be built at Full Sutton in the East Riding of Yorkshire, which is designed to house 1,440 male inmates (below left). This follows the £253 million the Government has already spent on the HMP Five Wells project in Wellingborough (below right), which is expected to be completed this year, and the HMP Glen Parva project in Leicestershire, where costs have so far reached £286 million.


Built with public money, these ‘mega prisons’ will be privately run by the same corporations to which the construction and running of the UK biosecurity state has been outsourced by the UK Government. These include Serco, the UK provider of public services in prisons, border security, military defence and information technology, which in 2013 was found by the prison inspectorate to be locking 60 per cent of prisoners in their cells up to 23 hours per day in HMP Thameside, was accused of covering up sexual abuse in the Yarl’s Wood Immigration centre, and in 2019 was fined £22.9 million by the Serious Fraud Office for charging the Government for electronically tagging people who were dead, in gaol, or outside the UK, yet in 2020 was awarded the contract to run the £37 billion ‘NHS Test and Trace’ programme that was renewed in June 2021; G4S, the UK’s largest security services company, which has been accused of using detained immigrants as cheap labour in prisons, extreme misconduct in child custodial institutions in the UK and the US, of collaborating in police telephone data manipulation, and which has also been awarded contracts to operate 21 COVID-19 ‘vaccination’ centres in the UK; and Sodexo, the French food services and facilities management company and one of the world’s largest multinational corporations, whose subsidiary, Sodexo Justice Services, was criticised by the UK Ministry of Justice in February 2019 for failing to prevent repeated and systemic breaches of the human rights of inmates at HMP Peterborough, including illegal strip-searches of prisoners and leaving a woman to give birth alone in her cell without any kind of medical support, and which as of July 2021 runs 30 per cent of all COVID-19 testing centres in the UK.
This, however, is only the first step in fulfilling the Government’s promise, which it announced in November 2020, 9 months into the coronavirus crisis, to allocate £4 billion in order to create sufficient prisons to incarcerate 18,000 new inmates, plus an additional £275 million to recruit 20,000 more police officers. For what new crimes this 23 per cent increase in the prison population of the UK and 13 per cent increase in police officers is warranted or anticipated in the UK biosecurity state the Government did not say; but the warnings in the House of Commons briefing issued by the Home Secretary, the Commissioner of the Metropolitan Police Service, the Chairman of the National Police Chiefs’ Council and the College of Policing on the enforcing of coronavirus-justified restrictions should be sufficient warning of what awaits the non-compliant. We must presume that Serco, G4S, Sodexo and the other corporations to which the UK Government has outsourced our former public services will apply the same standards of incompetence, ruthlessness, abuse of human rights, breaches of data privacy, exploitation of inmate labour, monopoly of Government contracts and financial opportunism to tracking, tracing, testing, quarantining and imprisoning those former citizens who fail to comply with the regulations or meet the obligations of citizenship in the UK biosecurity state.
As I’ve said before, and which I hope this summary of the powers, inducements and obligations made into law without legislative scrutiny, evidence of proportionality or assessment of their impact under this medically fictitious and politically declared emergency period proves: the progressive removal of the rights and freedoms of 68 million UK citizens isn’t the unfortunate consequence of the failure of coronavirus-justified regulations and programmes to halt the spread and impact of a new disease that threatens the public health of the UK. On the contrary, it is the product of the success of 18 months of regulations and programmes in implementing the revolutionary transition from the neoliberalism that has dominated the economy, politics, laws and culture of the UK for the past 40 years into the constitutional dictatorship of the UK biosecurity state in 2021.
In the third and final part of this article, I’ll look at what we must do to oppose the medical fundamentalism of the coronavirus ‘pandemic’, reassert our intellectual rights to question the orthodoxies of the New Normal it has been used to enforce, and, above all, resist and overthrow the totalitarian future prepared for us, and which is so nearly our present.
Simon Elmer
Architects for Social Housing
Collections of writings by the same author about the UK biosecurity state :
Brave New World: Expanding the UK Biosecurity State through the Winter of 2020-2021
COVID-19: Implementing the UK Biosecurity State
Architects for Social Housing is a Community Interest Company (no. 10383452). Although we occasionally receive minimal fees for our design work, the majority of what we do is unpaid and we have no source of public funding. If you would like to support our work financially, including the research for these articles, please make a donation through PayPal:
![]()

Dear Mr Elmer,
What a stupendous effort! Thank you for taking the time to put all this together.
I am not in the UK, but we have a very similar situation here. In fact, we’ve just had a federal election, and our head of government — the architect of said election, which was called for no good reason halfway into the PM’s term, cost the country some $600 million, and took place even as jurisdictions have been busy implementing vaccine passports to protect the public from a ‘fourth wave’ — spent a good chunk of his campaign demonising unvaccinated people such as myself.
I know that you consider neoliberalism to be the culprit behind the rise of the biosecurity state. However, the rise of the biosecurity state is happening all around the world, in countries that are in many ways antithetical to the Western world (for example, China and Russia). Russia, for instance, does not have ‘Big Pharma’, and it has come out with its own vaccines. Moscow tried to implement the use of vaccine passports in the summer, though apparently with little success. Without downplaying the role of corporate greed and neoliberalism in all this, are you willing to consider the possibility that modern society has simply reached a historical stage at which it desires the application of biopolitics for its further development? I used to think that all the people complying with COVID restrictions were doing it out of fear. While I believe this is still the case to a considerable extent, I have come to believe that many people are actually quite comfortable with living in a biosecurity state, for whatever reasons. (This is in no way to suggest that we should submit to the current situation and resign ourselves to biopolitics.) I would be interested in your thoughts.
Thank you for your good work.
Also, kudos for reminding your readers that the word ‘refusenik’ originally meant something other than what many people think it means!
LikeLike
“Russia, for instance, does not have ‘Big Pharma’, and it has come out with its own vaccines”.
Actually, I think the relationship between Russia and global corporations is an extremely tense and unclear one. In the 1990s, the US government had reduced Russia to such abject passivity and supineness that Western (mainly US) corporations rushed in and ravaged the country without mercy.
Then along came Mr Putin, who essentially restored the authority and sovereignty of the Russian government. At the national level, Mr Putin’s government has succeeded admirably in keeping Western interference at arm’s length. But global corporations worm their way in most insidiously… If Moscow was the part of Russia that took most enthusiastically to repressive measures and “vaccination”, that may well be because industrialised cities are where the greatest concentration of “Atlanticists”, “democrats” and stooges of corporations and Western governments are to be found.
The most hopeful fact is that a large majority of the Russian people seems to be well aware of the selfish, cynical goals of “the West”, and determined not to give way to them. It has often been remarked by well-informed observers that the West should not wish for Mr Putin’s retirement or overthrow, as his successor would almost certainly be far more “hard-line” and far less friendly towards the West.
As for China, it is even more of a mystery. One can only hope that the government of Mr Xi has a firm grip on the situation; it is definitely supported by a large majority of Chinese citizens. Mr Xi’s emphasis on fighting corruption in every form would, of course, also serve as protection against global corporations, which use corruption to extend their influence into countries where they are unwelcome.
It has also been remarked that the apparently extreme and illiberal reactions of the Chinese government to the virus might well be explained if they thought that they were under attack by actual biological warfare. Knowing Washington’s track record and values, that would not be in the least surprising. The Russians, too, may have chosen to react cautiously and asusme, until proven otherwise, that they were under attack.
LikeLike
Given that the bulk of this article is an attack on growing totalitarianism in the UK, to “hope that the government of Mr Xi has a firm grip on the situation” implies support for a state which is the model of totalitarianism for the rest of the world, in particular its Social Credit system, which the Health Passes in other countries is a a step towards. A deeply shameful comment.
LikeLike
I agree with ‘samfanto’ here. Mr Elmer’s long article provides a compelling analysis of the continued erosion of civil liberties in the UK (and in many other Western countries), and it’s curious to see some readers, who are supposedly sympathetic to the message, express hope that the ‘government of Mr Xi has a firm grip on the situation’. Ah, the government of Mr Xi, that antidote to our malaise, that champion of human rights, that crusader for freedoms!
As always, people’s beliefs, biases and prejudices shape their response to the current moment. Marxists will tell you the culprit is neoliberalism and transnational corporations. Anarchists will point the finger at the institution of government. Anti-Semites will rant about George Soros and the ‘Zionists’. Hardcore right-wingers will blame China and the left. Et cetera. Instead of aspiring to intellectual honesty, people simply use the ongoing crisis to feed their worldviews and advance their ideas. The more primitive the people, the more risible the ideas.
LikeLike
Hello Lord Covfefe, you might be interested in my new book, The Road to Fascism: For a Critique of the Global Biosecurity State, which I’ve been working on since February this year and published today. It’s available as a print-on-demand book in hardback and paperback editions (with an e-book forthcoming). Please click on this link for the contents page, my preface and purchase options. Best wishes. https://architectsforsocialhousing.co.uk/2022/09/28/the-road-to-fascism-for-a-critique-of-the-global-biosecurity-state/
LikeLike
About the Nuremberg code, this text I wrote back in June adds some nuance (from an anti-capitalist libertarian perspective) to the bits you mention in this long article: https://dialectical-delinquents.com/covid1984-latest/33239-2/
LikeLike
Hello Samfanto, you might be interested in my new book, The Road to Fascism: For a Critique of the Global Biosecurity State, which I’ve been working on since February this year and published today. It’s available as a print-on-demand book in hardback and paperback editions (with an e-book forthcoming). Please click on this link for the contents page, my preface and purchase options. Best wishes. https://architectsforsocialhousing.co.uk/2022/09/28/the-road-to-fascism-for-a-critique-of-the-global-biosecurity-state/
LikeLike
“No cause of death was listed on Jacob’s death certificate”.
Surely that is flagrantly illegal?
LikeLike